

The Impact of Mental Stress on Cardiovascular Health-Part II
- PMID: 35956022
- PMCID: PMC9369438
- DOI: 10.3390/jcm11154405
The Impact of Mental Stress on Cardiovascular Health-Part II
Abstract
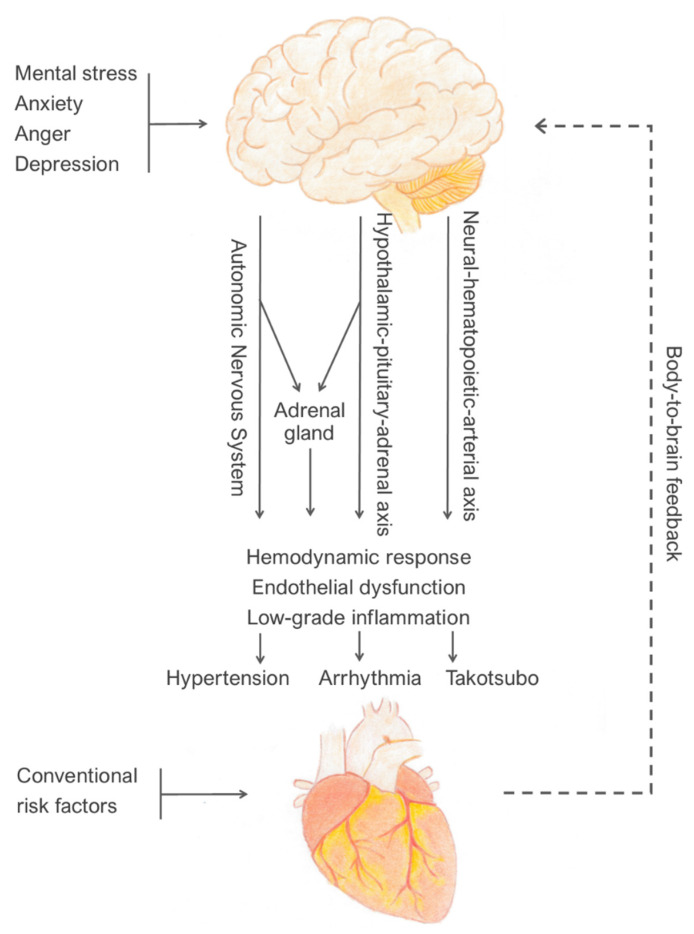
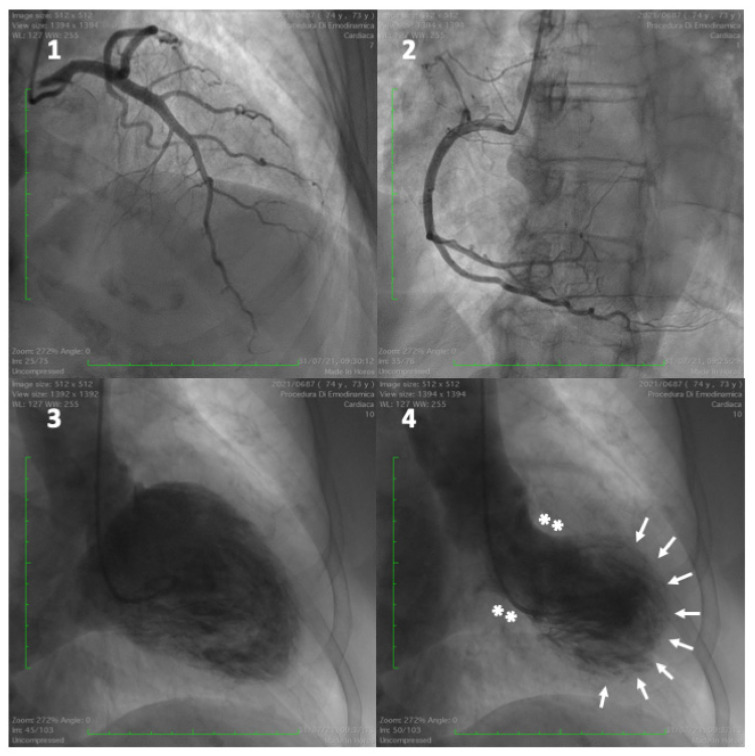
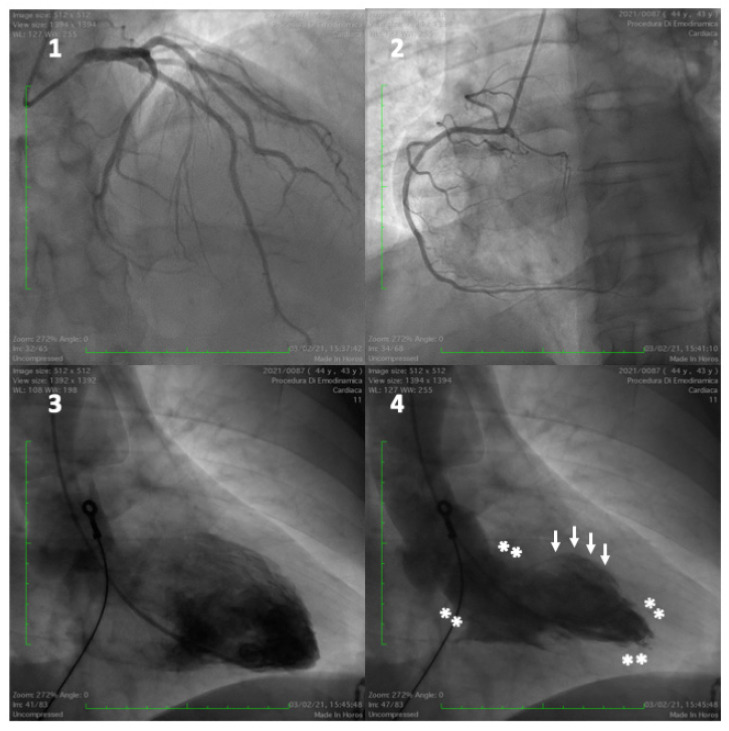
Endothelial dysfunction is one of the earliest manifestations of atherosclerosis, contributing to its development and progression. Mental stress induces endothelial dysfunction through increased activity of the sympathetic nervous system, release of corticotropin-releasing hormone from the hypothalamus, inhibition of nitric oxide (NO) synthesis by cortisol, and increased levels of pro-inflammatory cytokines. Mental-stress-induced increased output of the sympathetic nervous system and concomitant withdrawal of the parasympathetic inflammatory reflex results in systemic inflammation and activation of a neural-hematopoietic-arterial axis. This includes the brainstem and subcortical regions network, bone marrow activation, release of leukocytes into the circulation and their migration to the arterial wall and atherosclerotic plaques. Low-grade, sterile inflammation is involved in all steps of atherogenesis, from coronary plaque formation to destabilisation and rupture. Increased sympathetic tone may cause arterial smooth-muscle-cell proliferation, resulting in vascular hypertrophy, thus contributing to the development of hypertension. Emotional events also cause instability of cardiac repolarisation due to brain lateralised imbalance of cardiac autonomic nervous stimulation, which may lead to asymmetric repolarisation and arrhythmia. Acute emotional stress can also provoke severe catecholamine release, leading to direct myocyte injury due to calcium overload, known as myocytolysis, coronary microvascular vasoconstriction, and an increase in left ventricular afterload. These changes can trigger a heart failure syndrome mimicking acute myocardial infarction, characterised by transient left ventricular dysfunction and apical ballooning, known as stress (Takotsubo) cardiomyopathy. Women are more prone than men to develop mental-stress-induced myocardial ischemia (MSIMI), probably reflecting gender differences in brain activation patterns during mental stress. Although guidelines on CV prevention recognise psychosocial factors as risk modifiers to improve risk prediction and decision making, the evidence that their assessment and treatment will prevent CAD needs further evaluation.
Keywords: Takotsubo; arrhythmia; endothelial dysfunction; hypertension; mental stress; systemic inflammation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Yusuf S., Hawken S., Ôunpuu S., Dans T., Avezum A., Lanas F., McQueen M., Budaj A., Pais P., Varigos J., et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-Control study. Lancet. 2004;364:937–952. doi: 10.1016/S0140-6736(04)17018-9. - DOI - PubMed
-
- Rosengren A., Hawken S., Ôunpuu S., Sliwa K., Zubaid M., Almahmeed W.A., Blackett K.N., Sitthi-amorn C., Sato H., Yusuf S. Association of psychosocial risk factors with risk of acute myocardial infarction in 11,119 cases and 13,648 controls from 52 countries (the INTERHEART study): Case-Control study. Lancet. 2004;364:953–962. doi: 10.1016/S0140-6736(04)17019-0. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
