

Effectiveness of a Multifaced Antibiotic Stewardship Program: A Pre-Post Study in Seven Italian ICUs
- PMID: 35956026
- PMCID: PMC9369193
- DOI: 10.3390/jcm11154409
Effectiveness of a Multifaced Antibiotic Stewardship Program: A Pre-Post Study in Seven Italian ICUs
Abstract
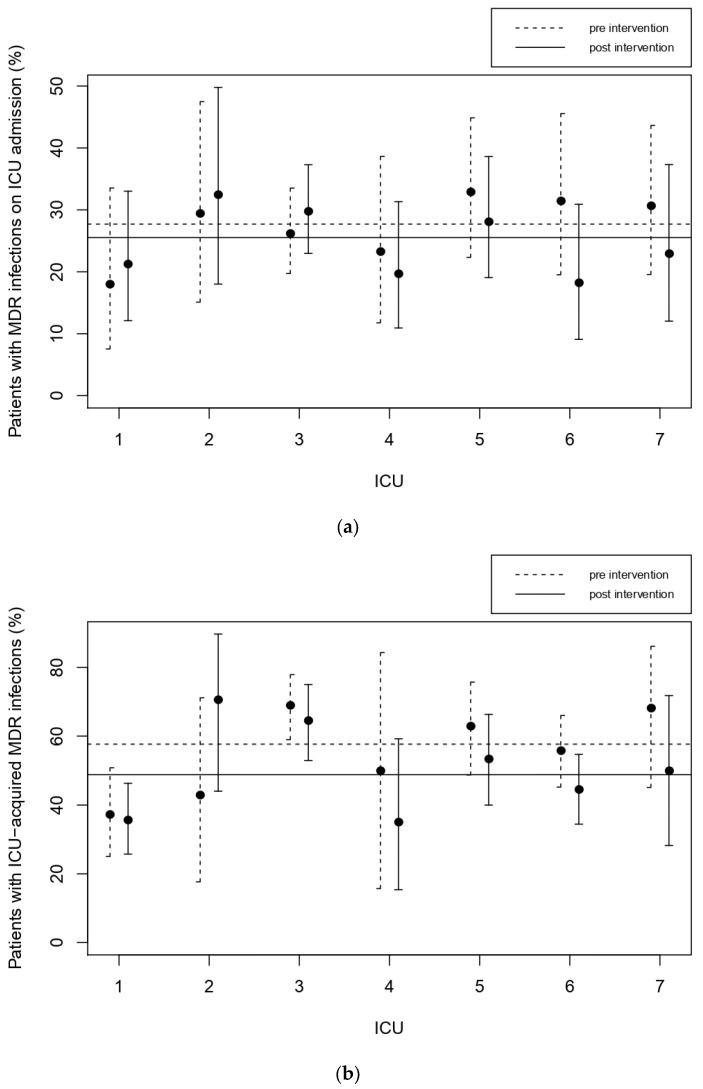
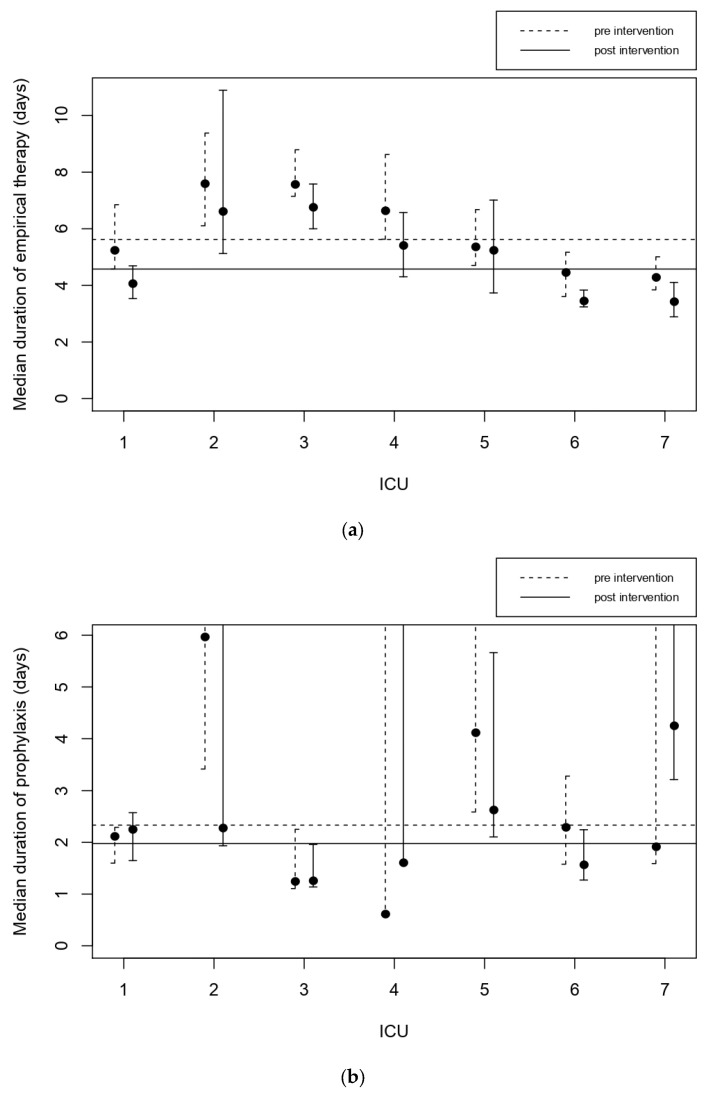
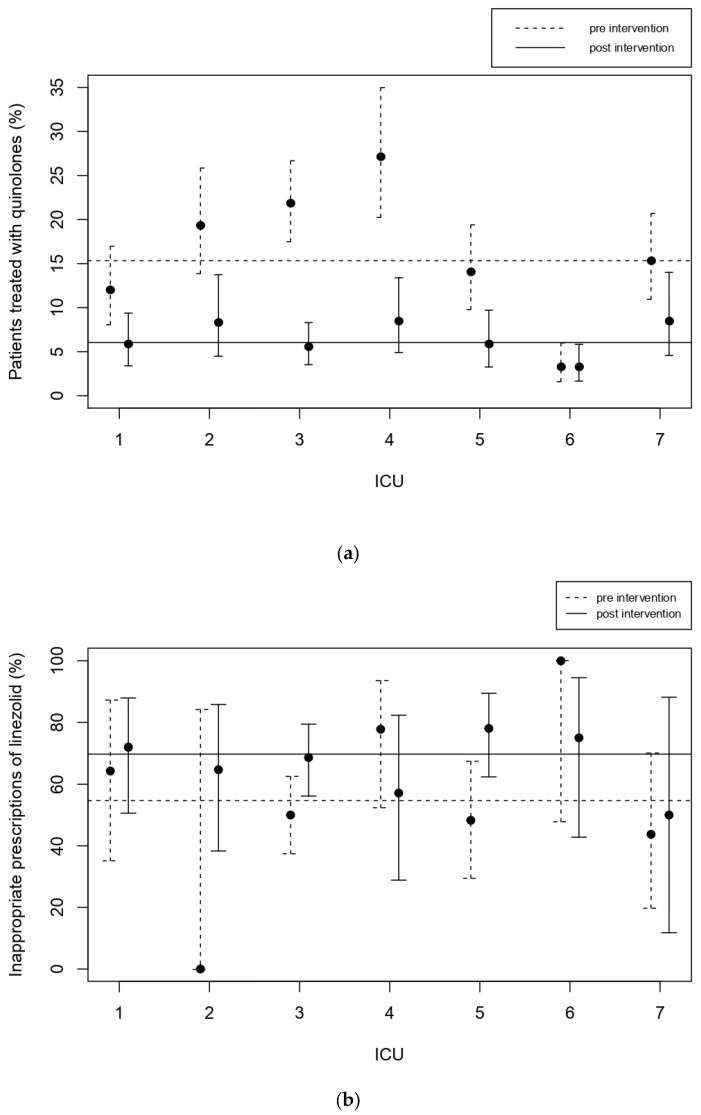
Multidrug resistance has become a serious threat for health, particularly in hospital-acquired infections. To improve patients’ safety and outcomes while maintaining the efficacy of antimicrobials, complex interventions are needed involving infection control and appropriate pharmacological treatments in antibiotic stewardship programs. We conducted a multicenter pre-post study to assess the impact of a stewardship program in seven Italian intensive care units (ICUs). Each ICU was visited by a multidisciplinary team involving clinicians, microbiologists, pharmacologists, infectious disease specialists, and data scientists. Interventions were targeted according to the characteristics of each unit. The effect of the program was measured with a panel of indicators computed with data from the MargheritaTre electronic health record. The median duration of empirical therapy decreased from 5.6 to 4.6 days and the use of quinolones dropped from 15.3% to 6%, both p < 0.001. The proportion of multi-drug-resistant bacteria (MDR) in ICU-acquired infections fell from 57.7% to 48.8%. ICU mortality and length of stay remained unchanged, indicating that reducing antibiotic administration did not harm patients’ safety. This study shows that our stewardship program successfully improved the management of infections. This suggests that policy makers should tackle multidrug resistance with a multidisciplinary approach based on continuous monitoring and personalised interventions.
Keywords: antibiotic stewardship; appropriateness of antibiotic; education in medicine; electronic health record; healthcare-associated infections; infection control; intensive care units; multidrug resistance.
Conflict of interest statement
The authors declare no conflict of interest influencing the representation or interpretation of reported research results.
Figures
References
-
- World Health Organization . WHO Report on Surveillance of Antibiotic Consumption: 2016–2018 Early Implementation. World Health Organization; Geneva, Switzerland: 2018.
-
- Davey P., Brown E., Charani E., Fenelon L., Gould I.M., Holmes A., Ramsay C.R., Wiffen P.J., Wilcox M. Interventions to Improve Antibiotic Prescribing Practices for Hospital Inpatients. Cochrane Database Syst. Rev. 2013;4:CD003543. - PubMed
