

Molecular Targets for Antibody-Based Anti-Biofilm Therapy in Infective Endocarditis
- PMID: 35956712
- PMCID: PMC9370930
- DOI: 10.3390/polym14153198
Molecular Targets for Antibody-Based Anti-Biofilm Therapy in Infective Endocarditis
Abstract
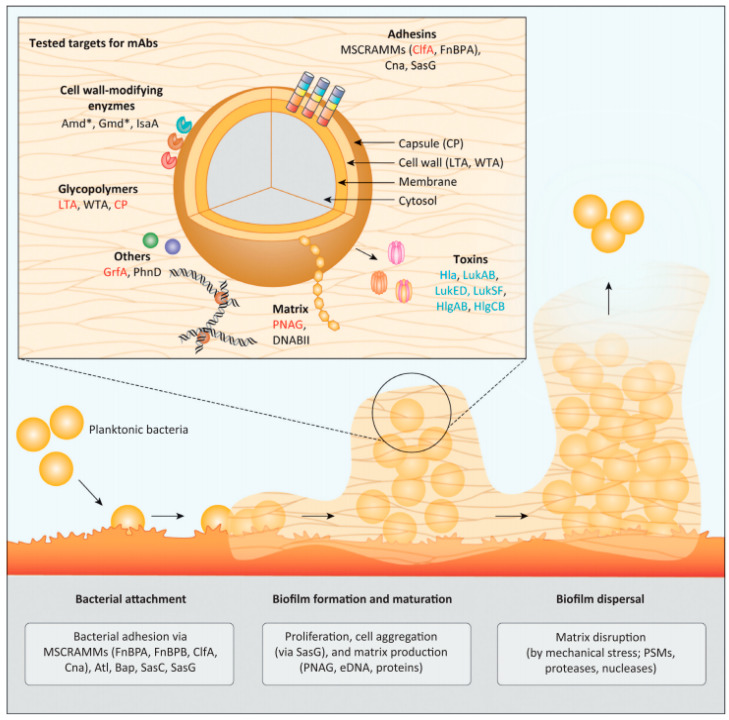
Infective endocarditis (IE) is a heart disease caused by the infection of heart valves, majorly caused by Staphilococcus aureus. IE is initiated by bacteria entering the blood circulation in favouring conditions (e.g., during invasive procedures). So far, the conventional antimicrobial strategies based on the usage of antibiotics remain the major intervention for treating IE. Nevertheless, the therapeutic efficacy of antibiotics in IE is limited not only by the bacterial drug resistance, but also by the formation of biofilms, which resist the penetration of antibiotics into bacterial cells. To overcome these drawbacks, the development of anti-biofilm treatments that can expose bacteria and make them more susceptible to the action of antibiotics, therefore resulting in reduced antimicrobial resistance, is urgently required. A series of anti-biofilm strategies have been developed, and this review will focus in particular on the development of anti-biofilm antibodies. Based on the results previously reported in the literature, several potential anti-biofilm targets are discussed, such as bacterial adhesins, biofilm matrix and bacterial toxins, covering their antigenic properties (with the identification of potential promising epitopes), functional mechanisms, as well as the antibodies already developed against these targets and, where feasible, their clinical translation.
Keywords: antibiotic resistance; antibodies; biofilms; epitopes; immunotherapy; infective endocarditis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures












Similar articles
-
Microbial biofilm correlates with an increased antibiotic tolerance and poor therapeutic outcome in infective endocarditis.BMC Microbiol. 2019 Oct 21;19(1):228. doi: 10.1186/s12866-019-1596-2. BMC Microbiol. 2019. PMID: 31638894 Free PMC article.
-
Bacterial biofilms in infective endocarditis: an in vitro model to investigate emerging technologies of antimicrobial cardiovascular device coatings.Clin Res Cardiol. 2021 Mar;110(3):323-331. doi: 10.1007/s00392-020-01669-y. Epub 2020 May 22. Clin Res Cardiol. 2021. PMID: 32444905 Free PMC article.
-
Anti-biofilm Approach in Infective Endocarditis Exposes New Treatment Strategies for Improved Outcome.Front Cell Dev Biol. 2021 Jun 18;9:643335. doi: 10.3389/fcell.2021.643335. eCollection 2021. Front Cell Dev Biol. 2021. PMID: 34222225 Free PMC article. Review.
-
The Assessment of Antimicrobial Resistance in Gram-Negative and Gram-Positive Infective Endocarditis: A Multicentric Retrospective Analysis.Medicina (Kaunas). 2023 Feb 24;59(3):457. doi: 10.3390/medicina59030457. Medicina (Kaunas). 2023. PMID: 36984458 Free PMC article.
-
Acinetobacter baumannii-induced infective endocarditis: new insights into pathophysiology and antibiotic resistance mechanisms.Future Microbiol. 2022 Nov;17:1335-1344. doi: 10.2217/fmb-2021-0279. Epub 2022 Sep 16. Future Microbiol. 2022. PMID: 36111747 Review.
Cited by
-
Understanding bacterial biofilms: From definition to treatment strategies.Front Cell Infect Microbiol. 2023 Apr 6;13:1137947. doi: 10.3389/fcimb.2023.1137947. eCollection 2023. Front Cell Infect Microbiol. 2023. PMID: 37091673 Free PMC article.
-
Revolutionizing Dentistry: Preclinical Insights and Future Applications of mRNA Vaccines in Dentistry-A Narrative Review.Dent J (Basel). 2025 Feb 13;13(2):79. doi: 10.3390/dj13020079. Dent J (Basel). 2025. PMID: 39996953 Free PMC article. Review.
-
Molecular Aspects of the Functioning of Pathogenic Bacteria Biofilm Based on Quorum Sensing (QS) Signal-Response System and Innovative Non-Antibiotic Strategies for Their Elimination.Int J Mol Sci. 2024 Feb 24;25(5):2655. doi: 10.3390/ijms25052655. Int J Mol Sci. 2024. PMID: 38473900 Free PMC article. Review.
-
C-terminal deletion of RelA protein is suggested as a possible cause of infective endocarditis recurrence with Enterococcus faecium.Antimicrob Agents Chemother. 2024 Mar 6;68(3):e0108323. doi: 10.1128/aac.01083-23. Epub 2024 Feb 13. Antimicrob Agents Chemother. 2024. PMID: 38349158 Free PMC article.
-
Whole-genome sequencing and biofilm gene characterization in multidrug-Resistant Staphylococcus aureus clinical strains.J Genet Eng Biotechnol. 2025 Sep;23(3):100521. doi: 10.1016/j.jgeb.2025.100521. Epub 2025 Jun 15. J Genet Eng Biotechnol. 2025. PMID: 40854640 Free PMC article.
References
-
- Pant S., Patel N.J., Deshmukh A., Golwala H., Patel N., Badheka A., Hirsch G.A., Mehta J.L. Trends in infective endocarditis incidence, microbiology, and valve replacement in the United States from 2000 to 2011. J. Am. Coll. Cardiol. 2015;65:2070–2076. doi: 10.1016/j.jacc.2015.03.518. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
