

Urine biochemistry assessment in the sequential evaluation of renal function: Time to think outside the box
- PMID: 35957852
- PMCID: PMC9360530
- DOI: 10.3389/fmed.2022.912877
Urine biochemistry assessment in the sequential evaluation of renal function: Time to think outside the box
Abstract
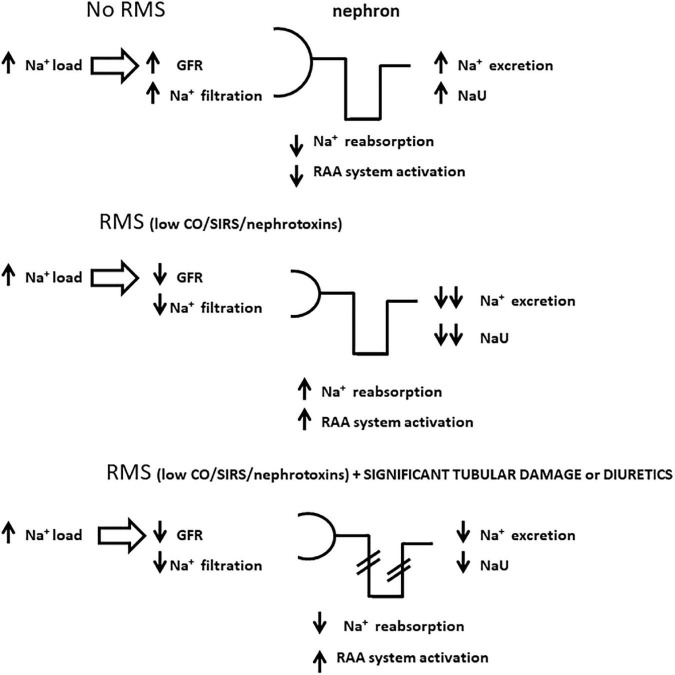
Urine biochemistry (UB) remains a controversial tool in acute kidney injury (AKI) monitoring, being considered to be of limited value both in terms of AKI diagnosis and prognosis. However, many criticisms can be made to the studies that have established the so called "pre-renal paradigm" (used for decades as the essential physiological basis for UB assessment in AKI) as well as to more recent studies suggesting that UB has no utility in daily clinical practice. The aim of this article is to describe our hypothesis on how to interpret simple and widely recognized urine biochemical parameters from a novel perspective, propose the rationale for their sequential assessment and demonstrate their usefulness in AKI monitoring, especially in the critical care setting.
Keywords: acute kidney injury; electrolytes; fractional excretion of potassium; monitoring; renal microcirculatory stress; urine; urine biochemistry; urine sodium.
Copyright © 2022 Maciel, Vitorio and Osawa.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
Introducing the "urine biochemical approach": an alternative tool for improving acute kidney injury monitoring in critically ill patients.Front Nephrol. 2025 Feb 19;5:1525551. doi: 10.3389/fneph.2025.1525551. eCollection 2025. Front Nephrol. 2025. PMID: 40046268 Free PMC article.
-
Urine biochemistry assessment in critically ill patients: controversies and future perspectives.J Clin Monit Comput. 2017 Jun;31(3):539-546. doi: 10.1007/s10877-016-9871-3. Epub 2016 Apr 1. J Clin Monit Comput. 2017. PMID: 27038161 Review.
-
Urine electrolyte measurement as a "window" into renal microcirculatory stress assessment in critically ill patients.J Crit Care. 2018 Dec;48:90-96. doi: 10.1016/j.jcrc.2018.08.011. Epub 2018 Aug 17. J Crit Care. 2018. PMID: 30176529 Review.
-
Urine biochemistry in septic and non-septic acute kidney injury: a prospective observational study.J Crit Care. 2013 Aug;28(4):371-8. doi: 10.1016/j.jcrc.2012.10.007. Epub 2012 Nov 14. J Crit Care. 2013. PMID: 23159144 Free PMC article.
-
Renal blood flow, fractional excretion of sodium and acute kidney injury: time for a new paradigm?Curr Opin Crit Care. 2012 Dec;18(6):585-92. doi: 10.1097/MCC.0b013e328358d480. Curr Opin Crit Care. 2012. PMID: 22954663 Review.
Cited by
-
Assessing donor kidney function: the role of CIRBP in predicting delayed graft function post-transplant.Front Immunol. 2025 Jan 17;15:1518279. doi: 10.3389/fimmu.2024.1518279. eCollection 2024. Front Immunol. 2025. PMID: 39896811 Free PMC article.
-
Optimizing Postoperative Acute Kidney Injury Monitoring Using a Urine Biochemical Approach-Time to Bring More Dynamism to Serum Creatinine Evaluation!Indian J Crit Care Med. 2024 Aug;28(8):729-733. doi: 10.5005/jp-journals-10071-24771. Epub 2024 Jul 31. Indian J Crit Care Med. 2024. PMID: 39239174 Free PMC article.
-
Plug-and-play protein biosensors using aptamer-regulated in vitro transcription.Nat Commun. 2024 Sep 12;15(1):7973. doi: 10.1038/s41467-024-51907-4. Nat Commun. 2024. PMID: 39266511 Free PMC article.
References
LinkOut - more resources
Full Text Sources