

Case Reports
doi: 10.1155/2022/5690844.
eCollection 2022.
Post-Myocardial Infarction Ventricular Septal Defect Successfully Treated with Impella as Bridge to Cardiac Transplantation
Affiliations
- PMID: 35958101
- PMCID: PMC9357800
- DOI: 10.1155/2022/5690844
Item in Clipboard
Case Reports
Post-Myocardial Infarction Ventricular Septal Defect Successfully Treated with Impella as Bridge to Cardiac Transplantation
Case Rep Cardiol.
.
Abstract
A 63-year-old female presented late with anterior ST-elevation myocardial infarction and cardiogenic shock. This was complicated by acute ventricular septal defect with large left-to-right shunt. An Impella CP was inserted on day seven with rapid haemodynamic improvement. This facilitated bridge to cardiac transplant on day twelve post-MI.
Copyright © 2022 Lauren Giudicatti et al.
Conflict of interest statement
The authors have no disclosures to declare.
Figures
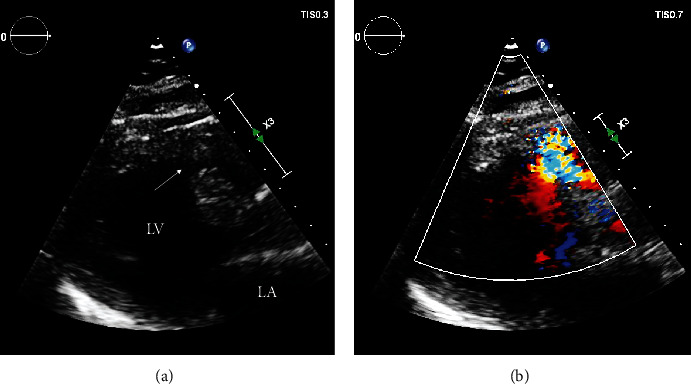
Transthoracic echocardiogram, parasternal long axis view, demonstrating a 1.3 cm muscular VSD in the basal anteroseptum ((a), arrow) with left-to-right shunting on colour Doppler (b).
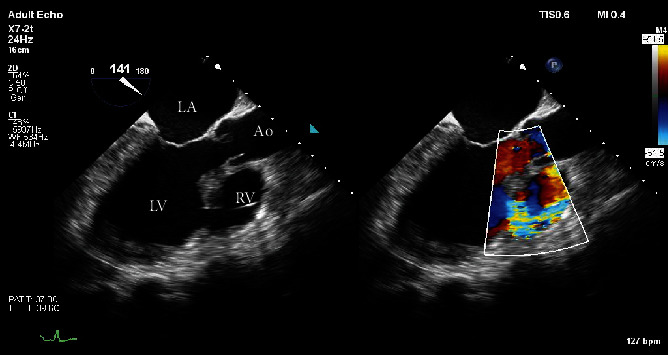
Transesophageal echocardiogram, midesophageal 3-chamber view taken whilst on Impella support, showing large VSD with left-to-right shunting on colour Doppler.
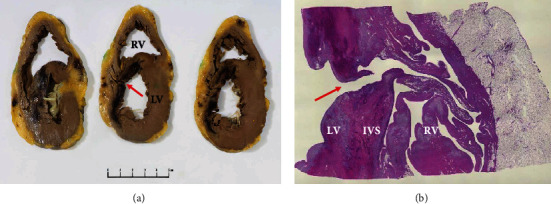
Explanted heart showing. (a) Cross-section through the basal (left) to apical (right) left ventricle (LV) demonstrating haemorrhagic infarct involving the interventricular septum (IVS) and anterior LV (asterisk). A defect is evident through the infarcted region of the IVS (arrow). (b) At low power, a full thickness defect is evident through the region of infarction (arrow), allowing communication from LV to RV, via a tortuous path.
Similar articles
-
Delayed Closure of Ventricular Septal Defect with Prolonged Mechanical Support.Eur J Case Rep Intern Med. 2024 May 13;11(6):004549. doi: 10.12890/2024_004549. eCollection 2024. Eur J Case Rep Intern Med. 2024. PMID: 38846674 Free PMC article.
-
Advantages of intraoperative implantation of Impella 5.5 SmartAssist in the Management of Acute Post-Infarction Ventricular Septal Defect with cardiogenic shock.J Cardiothorac Surg. 2021 May 17;16(1):132. doi: 10.1186/s13019-021-01513-y. J Cardiothorac Surg. 2021. PMID: 34001192 Free PMC article.
-
A case report of unexpected right-to-left shunt under mechanical support for post-infarction ventricular septal defect: evaluation with haemodynamic simulator.Eur Heart J Case Rep. 2021 Aug 31;5(8):ytab209. doi: 10.1093/ehjcr/ytab209. eCollection 2021 Aug. Eur Heart J Case Rep. 2021. PMID: 34514298 Free PMC article.
-
Percutaneous Transvalvular Microaxial Flow Pump Support in Cardiology.Circulation. 2022 Apr 19;145(16):1254-1284. doi: 10.1161/CIRCULATIONAHA.121.058229. Epub 2022 Apr 18. Circulation. 2022. PMID: 35436135 Review.
-
Percutaneous repair of post-myocardial infarction ventricular septal defect: current approaches and future perspectives.Tex Heart Inst J. 2014 Dec 1;41(6):613-9. doi: 10.14503/THIJ-13-3695. eCollection 2014 Dec. Tex Heart Inst J. 2014. PMID: 25593526 Free PMC article. Review.
Cited by
-
Improving Survival in Cardiogenic Shock-A Propensity Score-Matched Analysis of the Impact of an Institutional Allocation Protocol to Short-Term Mechanical Circulatory Support.Life (Basel). 2022 Nov 19;12(11):1931. doi: 10.3390/life12111931. Life (Basel). 2022. PMID: 36431066 Free PMC article.
-
The role of Impella in the pre-procedural management of post-infarct ventricular septal defect: a systematic review.Interdiscip Cardiovasc Thorac Surg. 2024 Dec 25;40(1):ivae212. doi: 10.1093/icvts/ivae212. Interdiscip Cardiovasc Thorac Surg. 2024. PMID: 39673774 Free PMC article.
-
Heart Transplantation in post-infarction ventricular septal rupture: Contemporary outcomes from the 2016-2021 National Inpatient Database.JHLT Open. 2025 Jun 3;9:100278. doi: 10.1016/j.jhlto.2025.100278. eCollection 2025 Aug. JHLT Open. 2025. PMID: 40606297 Free PMC article.
References
-
- Cinq-Mars A., Voisine P., Dagenais F., et al. Risk factors of mortality after surgical correction of ventricular septal defect following myocardial infarction: retrospective analysis and review of the literature. International Journal of Cardiology . 2016;206:27–36. doi: 10.1016/j.ijcard.2015.12.011. - DOI - PubMed
-
- Arnaoutakis G., Zhao Y., George T., Sciortino C., McCarthy P., Conte J. Surgical repair of ventricular septal defect after myocardial infarction: outcomes from the Society of Thoracic Surgeons National Database. The Annals of Thoracic Surgery . 2012;94(2):436–444. doi: 10.1016/j.athoracsur.2012.04.020. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
