

Comprehensive analysis of mutational profile and prognostic significance of complex glandular pattern in lung adenocarcinoma
- PMID: 35958332
- PMCID: PMC9359943
- DOI: 10.21037/tlcr-22-127
Comprehensive analysis of mutational profile and prognostic significance of complex glandular pattern in lung adenocarcinoma
Abstract
Background: Complex glandular pattern (CGP) was included as high-grade pattern in the new grading system proposed by The International Association for the Study of Lung Cancer. We aimed to investigate the mutational profile and validate the prognostic significance and proper cut-off value to distinguish the aggressive behavior of CGP.
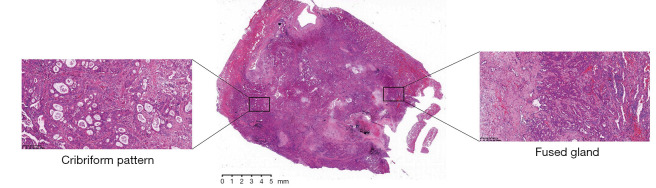
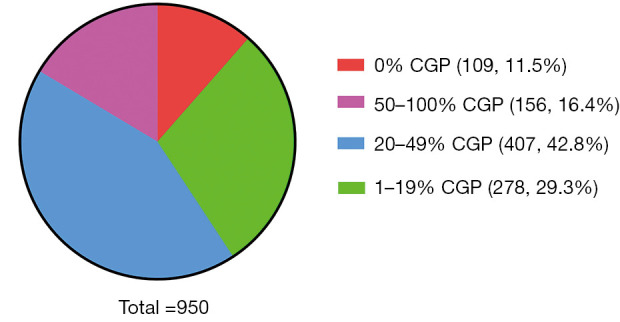
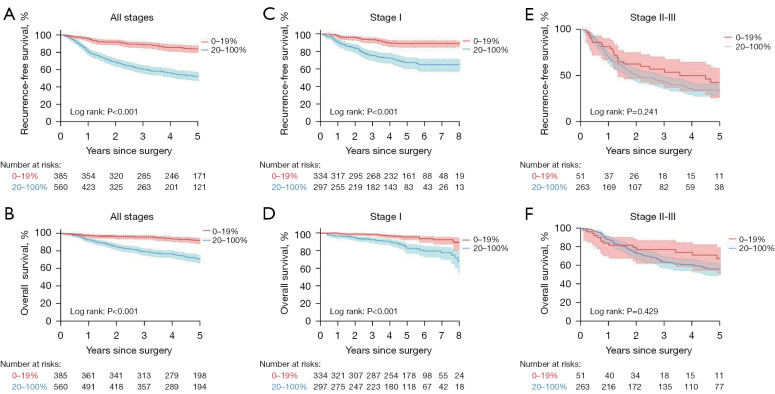
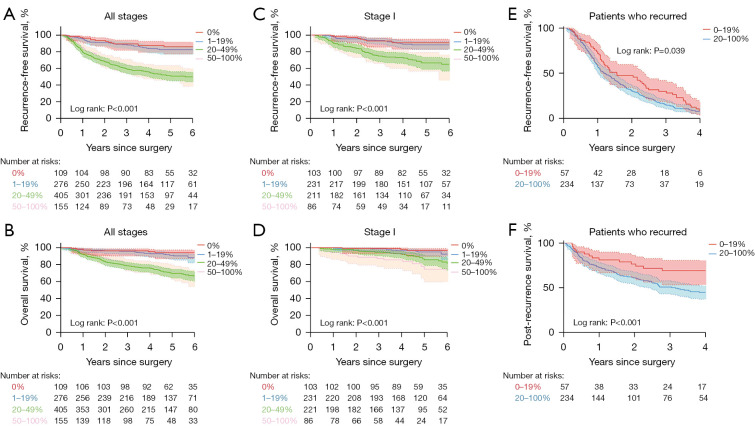
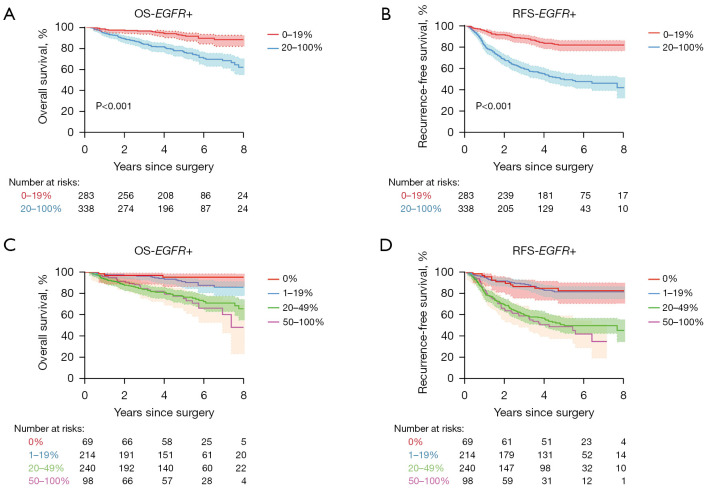
Methods: CGP was defined as nests of tumor cells with sieve-like perforation, fused glands with irregular borders or back-to-back glands without intervening stroma. Patients were categorized into four groups according to the percentage of CGP component (0%, 1-19%, 20-49%, 50-100%). Cox's proportional hazards model was applied to analyze recurrence free survival (RFS) and overall survival (OS).
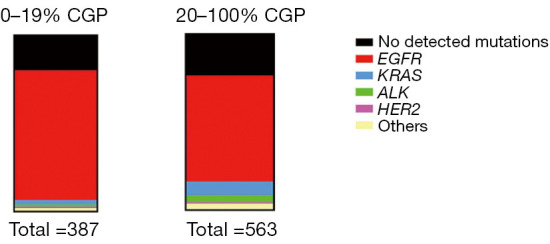
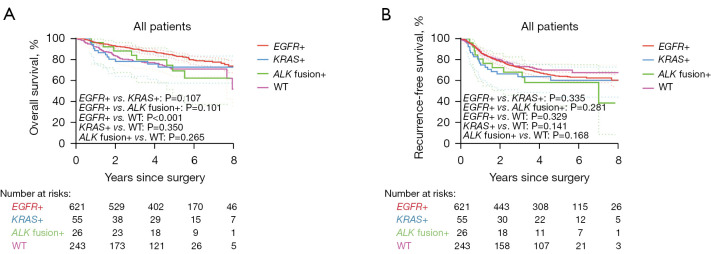
Results: A total of 950 patients with resected lung adenocarcinoma was enrolled. The most frequent driver mutation in this cohort was EGFR and was detected in 624 (65.7%) patients. EGFR mutation was more frequently observed in patients with <20% CGP than in patients with ≥20% CGP (73.6% vs. 60.2%), while KRAS mutation and ALK rearrangement was significantly associated with ≥20% CGP. Patients with 20% or greater CGP exhibited significant worse RFS (P<0.001) and OS (P<0.001) than their counterparts. Moreover, the multivariate Cox regression analysis confirmed that CGP (≥20%) was a risk factor for a worse RFS (P=0.001) and OS (P<0.001) independent of staging and gene mutation. Smaller portion of CGP (<20%) were comparable in RFS and OS to those without CGP (0%). There was also no significant difference in RFS and OS between the 20-49% and ≥50% group.
Conclusions: Our study provided mutational profile of patients with different CGP, validated CGP as a negative prognostic factor and provided extra evidences for the optimal cut-off value of CGP percentage.
Keywords: International Association for the Study of Lung Cancer grading system (IASLC grading system) grading system; complex glandular pattern (CGP); driver mutations; pulmonary adenocarcinoma.
2022 Translational Lung Cancer Research. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tlcr.amegroups.com/article/view/10.21037/tlcr-22-127/coif). The authors have no conflicts of interest to declare.
Figures
Comment in
-
Complex glandular pattern as an independent predictor of survival probability in lung adenocarcinoma.Transl Lung Cancer Res. 2022 Sep;11(9):1739-1741. doi: 10.21037/tlcr-22-513. Transl Lung Cancer Res. 2022. PMID: 36248342 Free PMC article. No abstract available.
References
-
- Kadota K, Kushida Y, Kagawa S, et al. Cribriform Subtype is an Independent Predictor of Recurrence and Survival After Adjustment for the Eighth Edition of TNM Staging System in Patients With Resected Lung Adenocarcinoma. J Thorac Oncol 2019;14:245-54. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous