

Natural course of pulmonary hyalinizing granuloma over a decade
- PMID: 35958350
- PMCID: PMC9358449
- DOI: 10.1016/j.rmcr.2022.101715
Natural course of pulmonary hyalinizing granuloma over a decade
Abstract
Background: Pulmonary hyalinizing granuloma (PHG) is a very rare pulmonary disease characterized by multiple fibrosclerotic inflammatory lung nodules. The disease is supposedly caused by an unusual immune response.
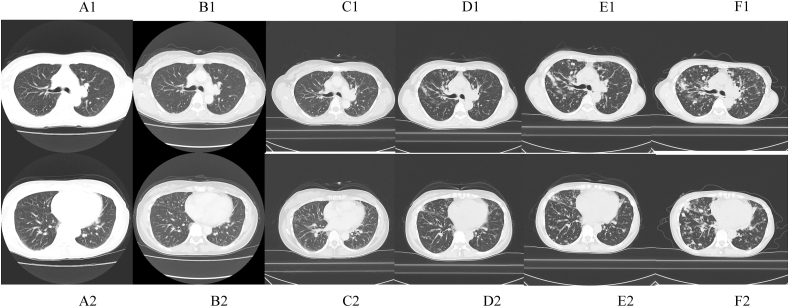
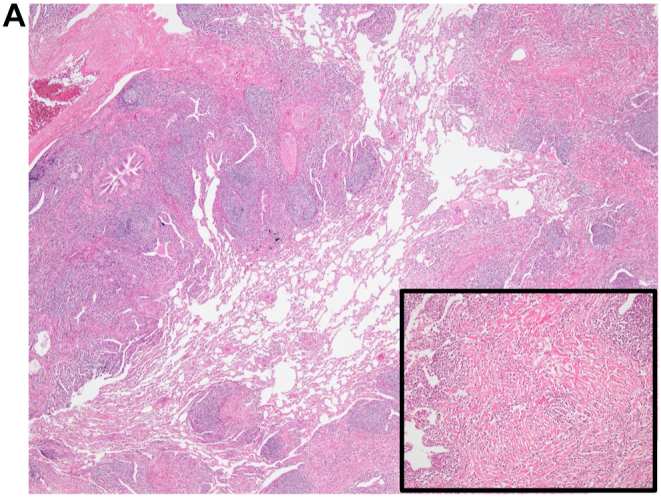
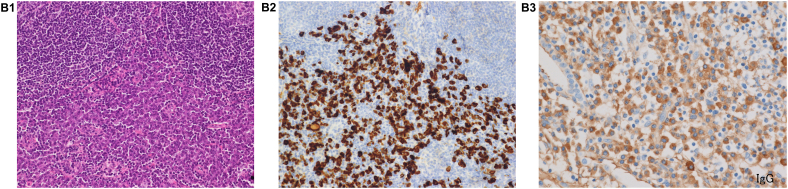
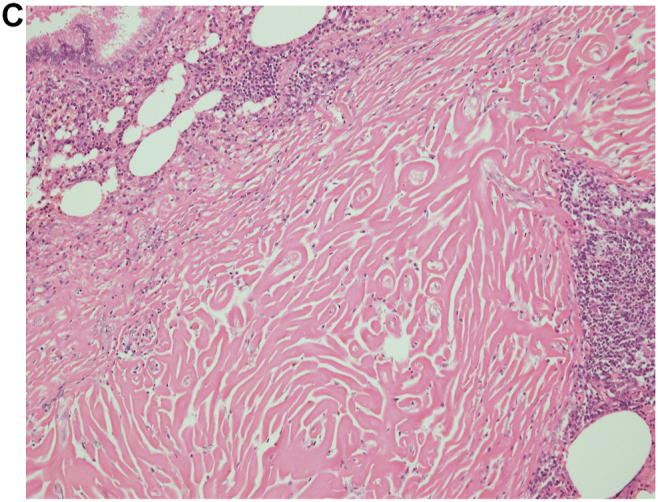
Case presentation: We present a case involving a 53-year-old female with a history of lumpectomy surgery due to invasive ductal carcinoma who was admitted for slowly progressive pulmonary nodules. The patient's elevated serum IgG4 level and the pathological findings obtained in surgical biopsy indicated IgG4-related lung disease. The nodules continued to enlarge despite administration of corticosteroid therapy, and we performed a second surgical biopsy to obtain a correct diagnosis. The pathological findings obtained in the second biopsy were different and consistent with the features of PHG.
Conclusions: In this report, the radiological follow-up data obtained after lumpectomy surgery demonstrate the very early stage of PHG and the following radiological changes over a decade, and the two surgical biopsies support us to realize the pathological change from previous diagnosed disease before PHG.
Keywords: IgG4-related lung disease; Interstitial pneumonia; Pulmonary hyalinizing granuloma.
© 2022 The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Lhote R., Haroche J., Duron L., et al. Pulmonary hyalinizing granuloma: a multicenter study of 5 new cases and review of the 135 cases of the literature. Immunol. Res. 2017 Feb;65(1):375–385. - PubMed
-
- Engleman P., Liebow A.A., Gmelich J., et al. Pulmonary hyalinizing granuloma. Am. Rev. Respir. Dis. 1977;115:997–1008. - PubMed
-
- Ussavarungsi K., Khoor A., Jolles H.I., et al. A 40-year-old woman with multiple pulmonary nodules. Pulmonary hyalinizing granuloma. Chest. 2014 Dec;146(6):e198–e203. - PubMed
-
- Na K.J., (1), Song S.Y., Kim J.H., et al. Subpleural pulmonary hyalinizing granuloma presenting as a solitary pulmonary nodule. J. Thorac. Oncol. 2007 Aug;2(8):777–779. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
