

Normal and abnormal development of the aortic valve and ascending aortic wall: a comprehensive overview of the embryology and pathology of the bicuspid aortic valve
- PMID: 35958528
- PMCID: PMC9357963
- DOI: 10.21037/acs-2021-bav-14
Normal and abnormal development of the aortic valve and ascending aortic wall: a comprehensive overview of the embryology and pathology of the bicuspid aortic valve
Abstract
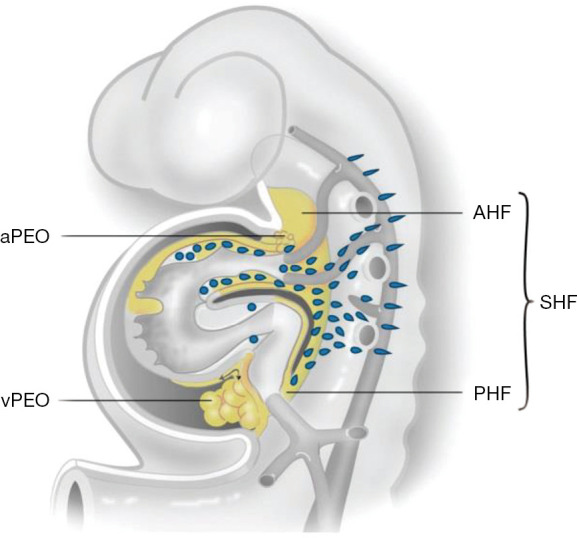
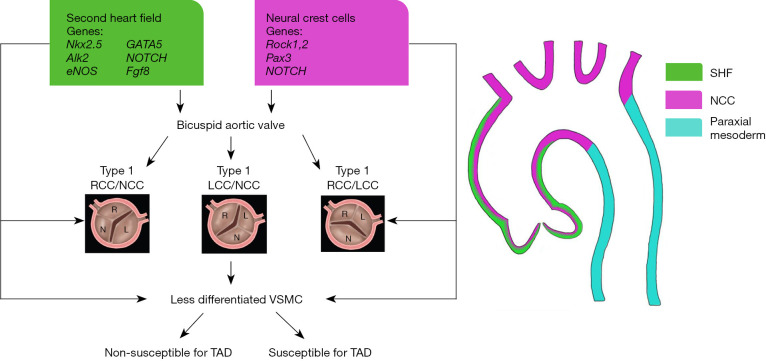
A bicuspid aortic valve (BAV) is the most prevalent congenital cardiac anomaly, in which the valve has only two leaflets, instead of the normal three. Patients with a BAV have an increased risk of aneurysm formation and the development of an aortic dissection. Vascular smooth muscle cells in both the non- and dilated aortic wall are characterized by a maturation defect in all BAV patients, as compared to patients with a tricuspid aortic valve, which can contribute to inherent developmental susceptibility. Besides structural abnormalities of the vascular wall, a turbulent blood flow, caused by bicuspid valve geometry, could expedite the pathological process in the aortic wall, leading to aortopathy. Although the risk for aortopathy is significant, not all BAV patients experience (acute) aortic complications in their lifespan, highlighting the complexity of the pathogenetic process. Recent studies have focused on the embryonic development of semilunar valves and the ascending aortic wall. Their findings highlight that a defect in the embryogenesis could not only explain the development of a malformed aortic valve but also the increased risk for ascending aorta and arch pathology. This review presents an overview of the normal and abnormal development of the aortic valve and the aortic wall: a common defect in early embryogenesis causes the development of a BAV and associated aortopathy.
Keywords: Bicuspid aortic valve (BAV); aortopathy; embryology; neural crest cells; pathology.
2022 Annals of Cardiothoracic Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources