

Speaking a common language: the international consensus on bicuspid aortic valve nomenclature and classification
- PMID: 35958544
- PMCID: PMC9357966
- DOI: 10.21037/acs-2022-bav-24
Speaking a common language: the international consensus on bicuspid aortic valve nomenclature and classification
Abstract
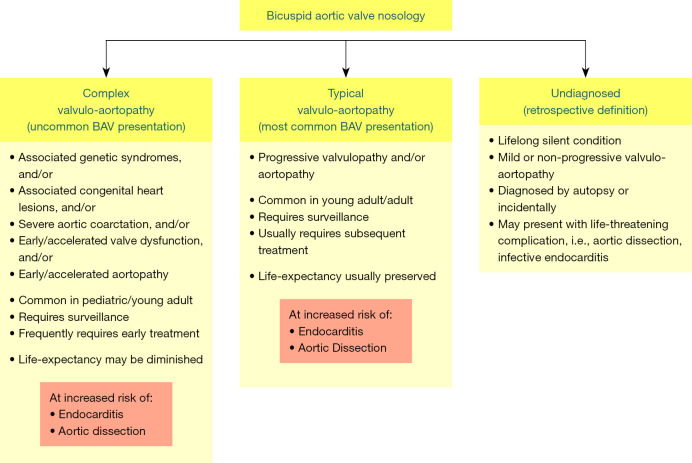
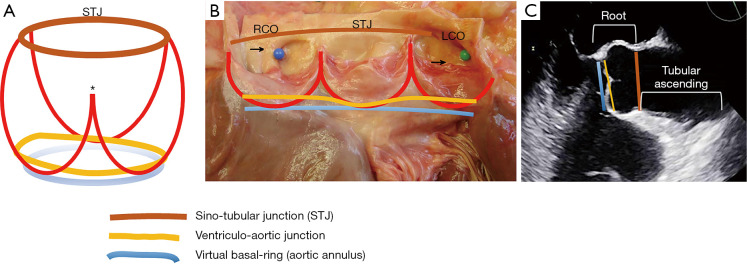
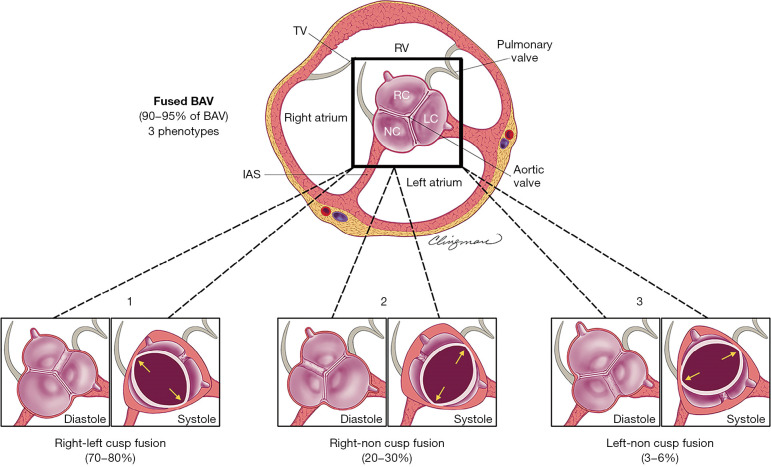
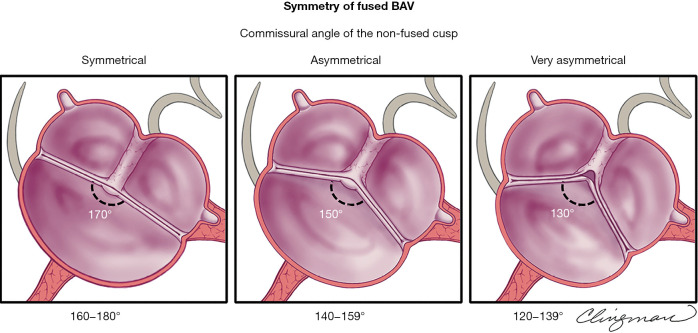
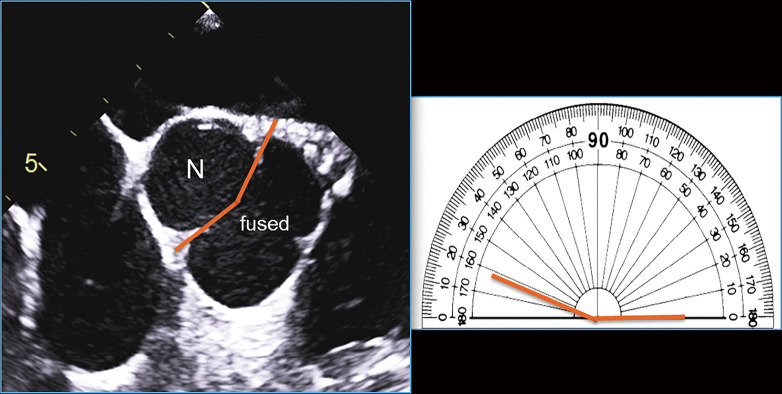
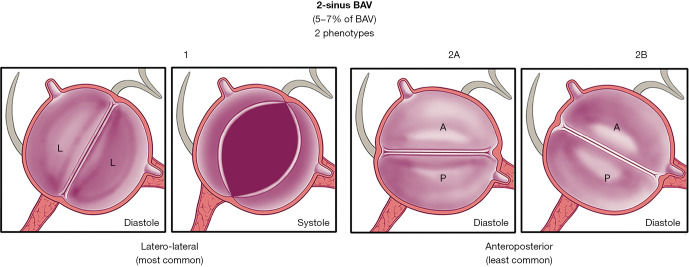
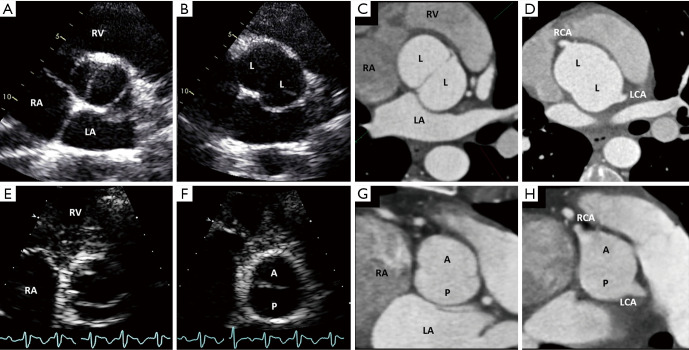
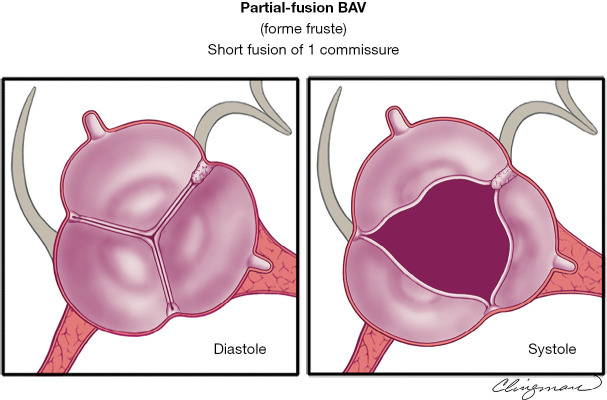
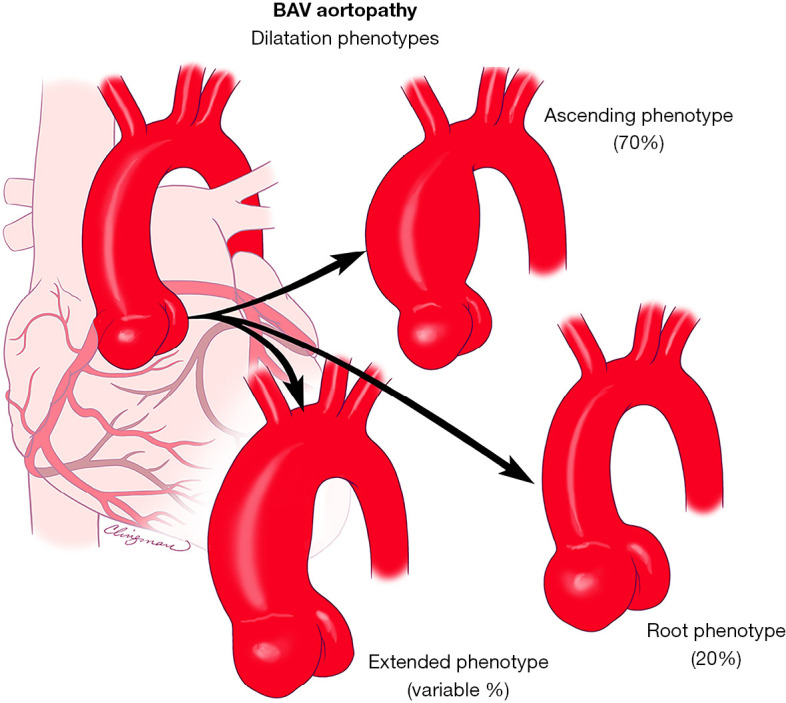
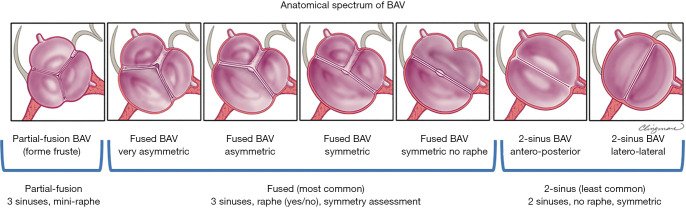
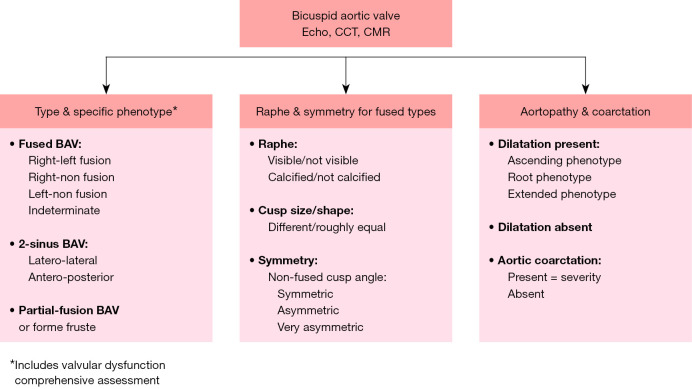
The congenital bicuspid aortic valve (BAV) condition is a valvulo-aortopathy with heterogeneous phenotypic expressions and clinical outcomes. A multitude of pre-existing classification systems, some extensive and some succinct, utilize combinations of numbers and/or letters to describe the condition. These diverse nomenclature systems are used according to the random preference of clinicians and researchers, generating confusion in clinical practice and research alike, effectively creating a barrier of communication at multiple levels. Based on imaging, pathology, surgery and clinical history evidence-based principles, and in utilizing the English language, the international nomenclature and classification consensus on the congenital BAV and its aortopathy offers a simple nosologic and phenotypic format that covers all possible phenotypes and clinical presentations of the bicuspid valvulo-aortopathy. From the nosology perspective, the valvulo-aortopathy has three major clinical presentations: (I) typical valvulo-aortopathy; (II) complex valvulo-aortopathy; and (III) undiagnosed or uncomplicated valvulo-aortopathy. From the valvular perspective, the congenital BAV has three major phenotypic expressions: (I) the fused BAV; (II) the 2-sinus BAV; and (III) the partial fusion (forme fruste) BAV. From the aortopathy perspective, the condition has three major phenotypic expressions: (I) ascending phenotype; (II) root phenotype; and (III) extended phenotypes. The international consensus is intended for universal use by Clinicians (pediatric and adult), echocardiography sonographers and physicians, cardiovascular advanced-imaging specialists, interventional cardiologists, cardiovascular surgeons, pathologists, geneticists and researchers encompassing clinical and basic research areas. When new landmark research is available, this international consensus may be subject to change in accordance with evidence-based data.
Keywords: Bicuspid aortic valve (BAV); aortopathy; classification; nomenclature.
2022 Annals of Cardiothoracic Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: Artivion (Consulting fees, speaker), and Mayo co-PI of PROACT Xa trial, Biostable Science and Engineering, Inc. (Consulting fees, speaker). The disclosures are unrelated to the keynote lecture.
Figures
References
-
- Michelena HI, Corte AD, Evangelista A, et al. International Consensus Statement on Nomenclature and Classification of the Congenital Bicuspid Aortic Valve and Its Aortopathy, for Clinical, Surgical, Interventional and Research Purposes. Radiol Cardiothorac Imaging 2021;3:e200496. 10.1148/ryct.2021200496 - DOI - PMC - PubMed
-
- Michelena HI, Della Corte A, Evangelista A, et al. International consensus statement on nomenclature and classification of the congenital bicuspid aortic valve and its aortopathy, for clinical, surgical, interventional and research purposes. J Thorac Cardiovasc Surg 2021;162:e383-414. 10.1016/j.jtcvs.2021.06.019 - DOI - PubMed
-
- Michelena HI, Della Corte A, Evangelista A, et al. International Consensus Statement on Nomenclature and Classification of the Congenital Bicuspid Aortic Valve and Its Aortopathy, for Clinical, Surgical, Interventional and Research Purposes. Ann Thorac Surg 2021;112:e203-35. 10.1016/j.athoracsur.2020.08.119 - DOI - PubMed
-
- Michelena HI, Della Corte A, Evangelista A, et al. International consensus statement on nomenclature and classification of the congenital bicuspid aortic valve and its aortopathy, for clinical, surgical, interventional and research purposes. Eur J Cardiothorac Surg 2021;60:448-76. 10.1093/ejcts/ezab038 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources