

Neuropathic Pain Relief after Surgical Neurolysis in Patients with Traumatic Brachial Plexus Injuries: A Preliminary Report
- PMID: 35958676
- PMCID: PMC9363225
- DOI: 10.1155/2022/5660462
Neuropathic Pain Relief after Surgical Neurolysis in Patients with Traumatic Brachial Plexus Injuries: A Preliminary Report
Abstract
Objective: To evaluate the usefulness of surgical neurolysis for neuropathic pain relief in patients with posttraumatic brachial plexus injury (BPI).
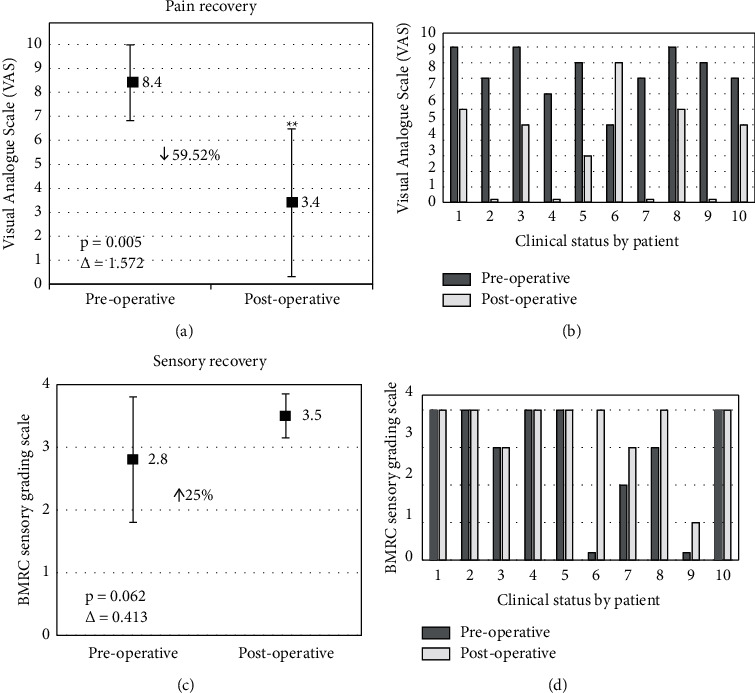
Methods: A prospective, longitudinal, nonrandomized, self-controlled before and after study was performed to evaluate the pain changes according to their intensity using the Visual Analogue Scale (VAS), and the sensory recovery after surgery using the British Medical Research Council (BMRC) scale for sensory recovery. To establish significant changes, a paired T-test was performed, and in order to determine the magnitude of these changes, an effect size was measured. α = 0.05.
Results: Ten patients were included with an average follow-up of 61.9 ± 53.62 months. The main mechanism of injury was vehicular trauma (70%). A significant decrease in pain after the surgical intervention was observed resulting from an average preoperative state according to VAS of 8.4 ± 1.58, to a postoperative state of 3.4 ± 3.27 (59.52%, p = 0.005, Δ = 1.572), added to a mean sensory improvement (25%) from 2.8 ± 1.62 to 3.5 ± 0.97 after surgery according to BMRC, without statistically significant changes (p=0.062), showing a moderate effect size (Δ = 0.413). Almost all patients showed improvement in the continuous and paroxysmal pattern of pain. No postoperative complications were observed. Discussion. These results suggest that in cases of BPI that originates from a compressive syndrome secondary to the posttraumatic fibrosis that surrounds the nerve structures causing strangulation and inducing hypernociception, the use of surgical neurolysis is an appropriate alternative for patients with medically refractory neuropathic pain.
Copyright © 2022 Armando Armas-Salazar et al.
Conflict of interest statement
The authors declare have no conflicts of interest to declare.
Figures
Similar articles
-
Neuropathic Pain and Positive Sensory Symptoms in Brachial Plexus Neuropathy: An Exploratory Study of Outcomes after Surgical Decompression and Proposal of a New Sensory Frequency of Symptoms Scale.J Integr Neurosci. 2023 Jan 17;22(1):25. doi: 10.31083/j.jin2201025. J Integr Neurosci. 2023. PMID: 36722242
-
Comparison of neuropathic pain characteristics associated with total brachial plexus injury before and after surgical repair: A retrospective study.Clin Neurol Neurosurg. 2020 Apr;191:105692. doi: 10.1016/j.clineuro.2020.105692. Epub 2020 Jan 23. Clin Neurol Neurosurg. 2020. PMID: 32087463
-
The effects of operative delay on the relief of neuropathic pain after injury to the brachial plexus: a review of 148 cases.J Bone Joint Surg Br. 2006 Jun;88(6):756-9. doi: 10.1302/0301-620X.88B6.16995. J Bone Joint Surg Br. 2006. PMID: 16720769
-
Thalamic deep brain stimulation for neuropathic pain after amputation or brachial plexus avulsion.Neurosurg Focus. 2013 Sep;35(3):E7. doi: 10.3171/2013.7.FOCUS1346. Neurosurg Focus. 2013. PMID: 23991820 Review.
-
[Pain management after post-traumatic brachial plexus lesions. Conservative and surgical therapy possibilities].Orthopade. 1997 Jul;26(7):621-5. doi: 10.1007/s001320050132. Orthopade. 1997. PMID: 9340591 Review. German.
Cited by
-
Review of rehabilitation protocols for brachial plexus injury.Front Neurol. 2023 Apr 17;14:1084223. doi: 10.3389/fneur.2023.1084223. eCollection 2023. Front Neurol. 2023. PMID: 37139070 Free PMC article. Review.
References
-
- Bannister K., Sachau J., Baron R. Neuropathic pain: mechanism-based therapeutics. Annual Review of Pharmacology and Toxicology . 2020;60:257–274. - PubMed
-
- Armas-Salazar A., García-Jerónimo A. I., Villegas-López F. A., Navarro-Olvera J. L., Carrillo-Ruiz J. D. Clinical outcomes report in different brachial plexus injury surgeries: a systematic review. Neurosurgical Review . 2022;45(1):411–419. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
