

Evaluation of pregnancy outcomes using medroxyprogesterone acetate versus gonadotropin-releasing hormone antagonist in ovarian stimulation: A retrospective cohort study
- PMID: 35958960
- PMCID: PMC9358237
- DOI: 10.18502/ijrm.v20i6.11445
Evaluation of pregnancy outcomes using medroxyprogesterone acetate versus gonadotropin-releasing hormone antagonist in ovarian stimulation: A retrospective cohort study
Abstract
Background: Limited studies have compared pregnancy outcomes with medroxyprogesterone acetate (MPA) vs. gonadotropin-releasing hormone antagonist (GnRH antagonist) in ovarian stimulation protocols. The results show heterogeneity.
Objective: This study aims to assess pregnancy outcomes with the use of MPA instead of GnRH antagonist for ovarian stimulation in donor-recipient cycles.
Materials and methods: This retrospective study was carried out from June 2016 to May 2019. The study included 250 donors receiving ovarian stimulation with 2 different protocols: group 1 (n = 109) receiving GnRH antagonist (0.25 mg/day) from the 5 or 6 day of menses and group 2 (n = 141) receiving MPA (10 mg/day) from the second day of menses. In 384 recipients, 2 good-quality blastocysts were transferred after endometrial preparation. The primary endpoint was live birth in recipients.
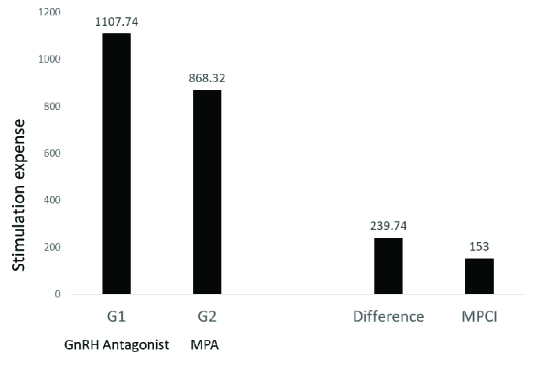
Results: The results showed that live birth was comparable in both recipient groups (59% vs. 60%, OR: 0.63, 95% CI: 0.13-2.99, p = 0.559). The number of live-born fetuses (adjusted OR: 0.57, 95% CI: 0.31-1.05, p 0.01) showed no significant difference in both groups. However, the implantation rate with twin sacs was significantly lower in group 2 (adjusted OR: 0.57, 95% CI: 0.33-0.99, p = 0.05). The regression analysis for good-quality blastocyst proportion was comparable (OR: 0.63, 95% CI: -4.33-5.60, p = 0.802) in both donor groups. The mean stimulation cost in group 2 was less than in group 1.
Conclusion: MPA had a comparable live birth and embryological outcomes in both groups. Oral administration makes it convenient, acceptable, and patient-friendly. Its cost-effectiveness and convenience open new possibilities in ovarian stimulation protocols.
Keywords: Gonadotropin-releasing hormone antagonist; Medroxyprogesterone acetate; Pregnancy outcomes.; Oocyte donation.
Copyright © 2022 Singh et al.
Figures
References
-
- Massin N. New stimulation regimens: Endogenous and exogenous progesterone use to block the LH surge during ovarian stimulation for IVF. Hum Reprod Update. 2017;23:211–220. - PubMed
-
- Kuang Y, Chen Q, Fu Y, Wang Y, Hong Q, Lyu Q, et al. Medroxyprogesterone acetate is an effective oral alternative for preventing premature luteinizing hormone surges in women undergoing controlled ovarian hyper stimulation for in vitro fertilization. Fertil Steril. 2015;104:62–70. - PubMed
-
- Guo YCh, Chen PY, Li TT, Jia L, Sun P, Zhu WS, et al. Different progestin-primed ovarian stimulation protocols in infertile women undergoing in vitro fertilization/intracytoplasmic sperm injection: An analysis of 1188 cycles. Arch Gynecol Obstet. 2019;299:1201–1212. - PubMed
-
- Yu Sh, Long H, Chang HYN, Liu Y, Gao H, Zhu J, et al. New application of dydrogesterone as a part of a progestin-primed ovarian stimulation protocol for IVF: A randomized controlled trial including 516 first IVF/ICSI cycles. Hum Reprod. 2018;33:229–237. - PubMed
-
- Zhu X, Ye H, Fu Y. Duphaston and human menopausal gonadotropin protocol in normally ovulatory women undergoing controlled ovarian hyperstimulation during in vitro fertilization/intracytoplasmic sperm injection treatments in combination with embryo cryopreservation. Fertil Steril. 2017;108:505–512. - PubMed
LinkOut - more resources
Full Text Sources