

Sparsely Granulated Corticotroph Pituitary Macroadenoma Presenting With Pituitary Apoplexy Resulting in Remission of Hypercortisolism
- PMID: 35959088
- PMCID: PMC9363514
- DOI: 10.1016/j.aace.2022.04.003
Sparsely Granulated Corticotroph Pituitary Macroadenoma Presenting With Pituitary Apoplexy Resulting in Remission of Hypercortisolism
Abstract
Objective: Pituitary corticotroph macroadenomas, which account for 7% to 23% of corticotroph adenomas, rarely present with apoplexy. This report aimed to describe a patient with a sparsely granulated corticotroph tumor (SGCT) presenting with apoplexy and remission of hypercortisolism.
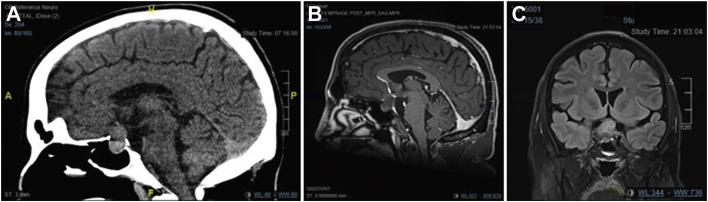
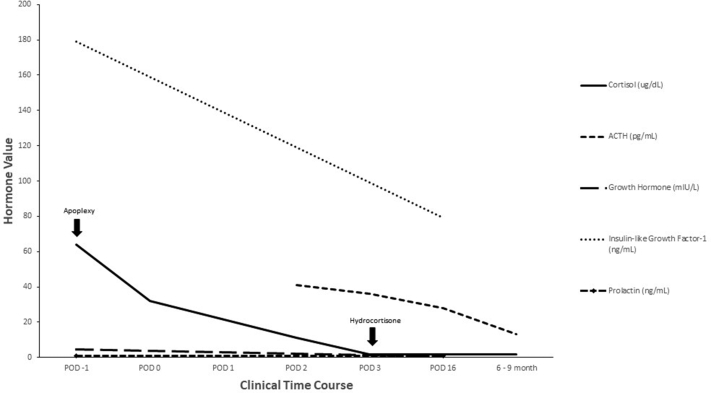
Case report: A 33-year-old male patient presented via ambulance with sudden onset of severe headache and nausea/vomiting. Physical examination revealed bitemporal hemianopsia, diplopia from right-sided third cranial nerve palsy, abdominal striae, facial plethora, and dorsal and supraclavicular fat pads. Magnetic resonance imaging demonstrated a 3.2-cm mass arising from the sella turcica with hemorrhage compressing the optic chiasm, extension into the sphenoid sinus and cavernous sinus. Initial investigations revealed a plasma cortisol level of 64.08 (reference range [RR], 2.36-17.05) mcg/dL. He underwent emergent transsphenoidal surgery. Pathology was diagnostic of SGCT. Postoperatively, the following laboratory findings were found: (1) cortisol level, <1.8 ug/dL (RR, 2.4-17); (2) adrenocorticotropic hormone level, 36 pg/mL (RR, 0-81); (3) thyroid-stimulating hormone level, 0.07 uIU/mL (RR, 0.36-3.74); (4) free thyroxine level, 1 ng/dL (RR, 0.8-1.5); (5) luteinizing hormone level, <1 mIU/mL (RR, 1-12); (6) follicle-stimulating hormone level, 1 mIU/mL (RR, 1-12); and (7) testosterone level, 28.8 ng/dL (RR, 219.2-905.6), with ongoing requirement for hydrocortisone, levothyroxine, testosterone replacement, and continued follow-up.
Discussion: Corticotroph adenomas are divided into densely granulated, sparsely granulated, and Crooke cell tumors. Sparsely granulated pattern is associated with a larger tumor size and decreased remission rate after surgery.
Conclusion: This report illustrates a rare case of hypercortisolism remission due to apoplexy of an SGCT with subsequent central adrenal insufficiency, hypothyroidism, and hypogonadism.
Keywords: ACTH, adrenocorticotropic hormone; CD, Cushing disease; Cushing disease; DGCT, densely granulated cell tumor; FSH, follicle-stimulating hormone; IGF-1, insulin-like growth factor 1; LH, luteinizing hormone; MRI, magnetic resonance imaging; RR, reference range; SGCT, sparsely granulated corticotroph tumor; TSH, thyroid-stimulating hormone; TSS, transsphenoidal surgery; pituitary apoplexy; pituitary macroadenoma; pituitary tumor; sparsely granulated corticotroph tumor.
© 2022 AACE. Published by Elsevier Inc.
Figures


Similar articles
-
Granulation Patterns of Functional Corticotroph Tumors Correlate with Tumor Size, Proliferative Activity, T2 Intensity-to-White Matter Ratio, and Postsurgical Early Biochemical Remission.Endocr Pathol. 2024 Sep;35(3):185-193. doi: 10.1007/s12022-024-09819-y. Epub 2024 Jul 24. Endocr Pathol. 2024. PMID: 39046680 Free PMC article.
-
Symptomatic Pituitary Metastasis as Initial Manifestation of Renal Cell Carcinoma: Case Report and Review of Literature.Case Rep Endocrinol. 2020 Aug 18;2020:8883864. doi: 10.1155/2020/8883864. eCollection 2020. Case Rep Endocrinol. 2020. PMID: 32908722 Free PMC article.
-
Synchronous Multiple Pituitary Neuroendocrine Tumors of Different Cell Lineages.Endocr Pathol. 2018 Dec;29(4):332-338. doi: 10.1007/s12022-018-9545-4. Endocr Pathol. 2018. PMID: 30215160
-
Clinically Silent Adrenocorticotropic Hormone-Positive Crooke Cell Adenoma: Case Report and Review of Literature.World Neurosurg. 2018 Nov;119:197-200. doi: 10.1016/j.wneu.2018.07.233. Epub 2018 Aug 2. World Neurosurg. 2018. PMID: 30077745 Review.
-
Gonadotropin-releasing hormone agonist-induced pituitary apoplexy in treatment of prostate cancer: case report and review of literature.Endocr Pract. 2007 Oct;13(6):642-6. doi: 10.4158/EP.13.6.642. Endocr Pract. 2007. PMID: 17954421 Review.
Cited by
-
Pituitary Apoplexy in Patients with Pituitary Neuroendocrine Tumors (PitNET).Biomedicines. 2023 Feb 23;11(3):680. doi: 10.3390/biomedicines11030680. Biomedicines. 2023. PMID: 36979658 Free PMC article. Review.
-
Granulation Patterns of Functional Corticotroph Tumors Correlate with Tumor Size, Proliferative Activity, T2 Intensity-to-White Matter Ratio, and Postsurgical Early Biochemical Remission.Endocr Pathol. 2024 Sep;35(3):185-193. doi: 10.1007/s12022-024-09819-y. Epub 2024 Jul 24. Endocr Pathol. 2024. PMID: 39046680 Free PMC article.
-
Editorial for July/August Issue of AACE Clinical Case Reports.AACE Clin Case Rep. 2022 Aug 2;8(4):147. doi: 10.1016/j.aace.2022.06.003. eCollection 2022 Jul-Aug. AACE Clin Case Rep. 2022. PMID: 35959089 Free PMC article. No abstract available.
-
Pituitary apoplexy in cushing's disease: a single center study and systematic literature review.Pituitary. 2024 Aug;27(4):335-344. doi: 10.1007/s11102-024-01411-1. Epub 2024 Jun 8. Pituitary. 2024. PMID: 38850401
-
Delayed diagnosis of the full triad autoimmune polyendocrine syndrome type 2 with adrenal crisis: a case report and literature review.Front Immunol. 2025 May 9;16:1563629. doi: 10.3389/fimmu.2025.1563629. eCollection 2025. Front Immunol. 2025. PMID: 40416965 Free PMC article. Review.
References
-
- Lindholm J., Juul S., Jørgensen J.O., et al. Incidence and late prognosis of Cushing's syndrome: a population-based study. J Clin Endocrinol Metab. 2001;86(1):117–123. - PubMed
-
- Etxabe J., Vazquez J.A. Morbidity and mortality in Cushing's disease: an epidemiological approach. Clin Endocrinol (Oxf) 1994;40(4):479–484. - PubMed
-
- Katznelson L., Bogan J.S., Trob J.R., et al. Biochemical assessment of Cushing's disease in patients with corticotroph macroadenomas. J Clin Endocrinol Metab. 1998;83(5):1619–1623. - PubMed
-
- Syro L.V., Rotondo F., Cusimano M.D., et al. Current status on histological classification in Cushing's disease. Pituitary. 2015;18(2):217–224. - PubMed
-
- Woo Y.S., Isidori A.M., Wat W.Z., et al. Clinical and biochemical characteristics of adrenocorticotropin-secreting macroadenomas. J Clin Endocrinol Metab. 2005;90(8):4963–4969. - PubMed
Publication types
LinkOut - more resources
Full Text Sources