

Sex-dimorphic gene effects on survival outcomes in people with coronary artery disease
- PMID: 35959094
- PMCID: PMC9365120
- DOI: 10.1016/j.ahjo.2022.100152
Sex-dimorphic gene effects on survival outcomes in people with coronary artery disease
Abstract
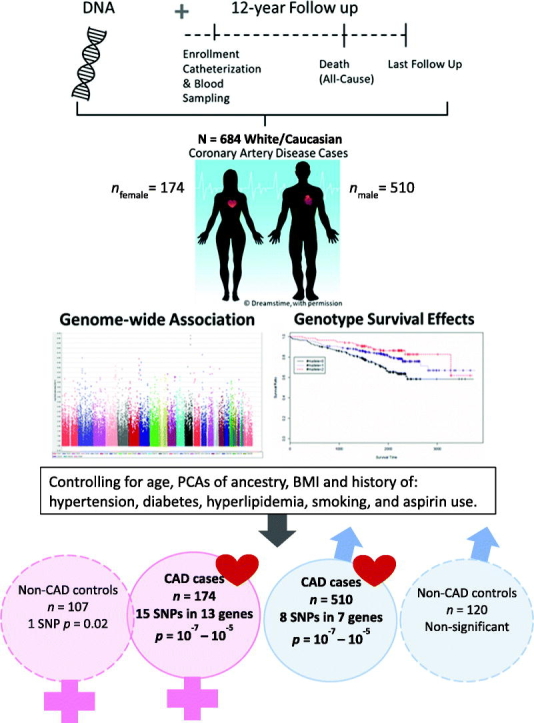
Background: Ischemic coronary heart disease (IHD) is the leading cause of death worldwide. Genetic variation is presumed to be a major factor underlying sex differences for IHD events, including mortality. The purpose of this study was to identify sex-specific candidate genes associated with all-cause mortality among people diagnosed with coronary artery disease (CAD).
Methods: We performed a sex-stratified, exploratory genome-wide association (GWAS) screen using existing data from CAD-diagnosed males (n = 510) and females (n = 174) who reported European ancestry from the Duke Catheterization Genetics biorepository. Extant genotype data for 785,945 autosomal SNPs generated with the Human Omni1-Quad BeadChip (Illumina, CA, USA) were analyzed using an additive inheritance model. We estimated instantaneous risk of all-cause mortality by genotype groups across the 11-year follow-up using Cox multivariate regression, covarying for age and genomic ancestry.
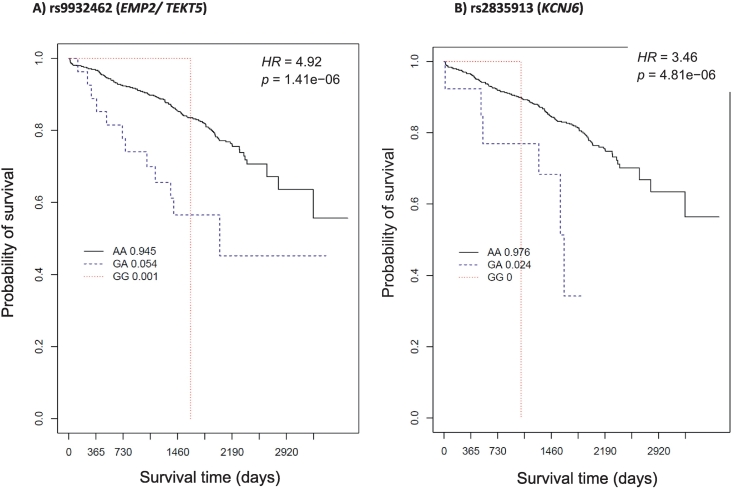
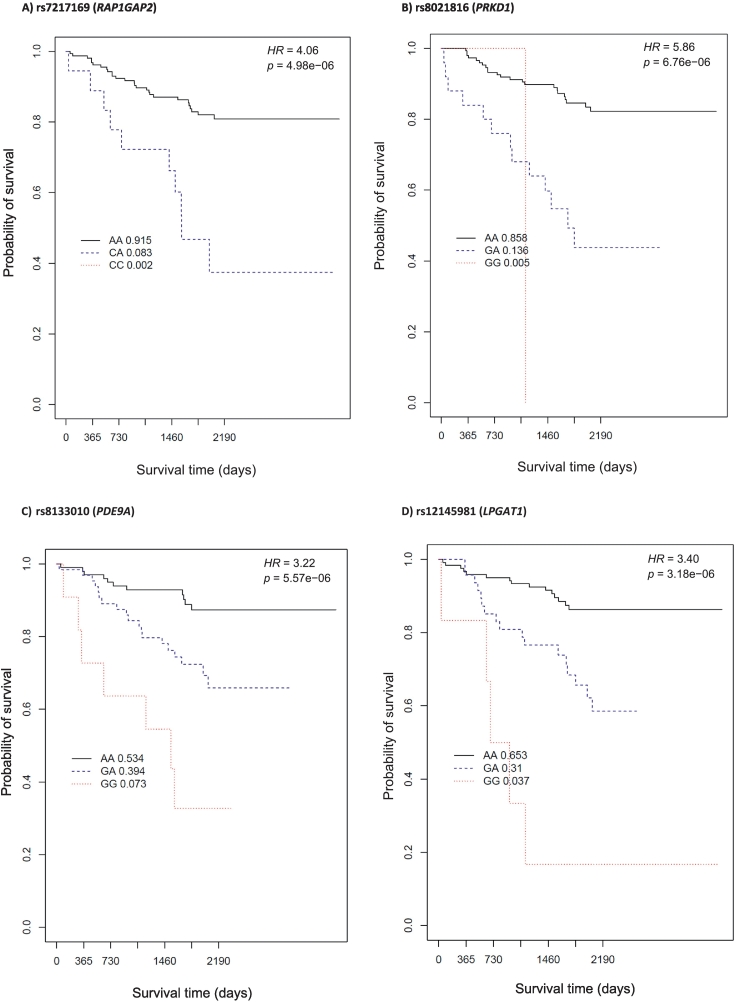
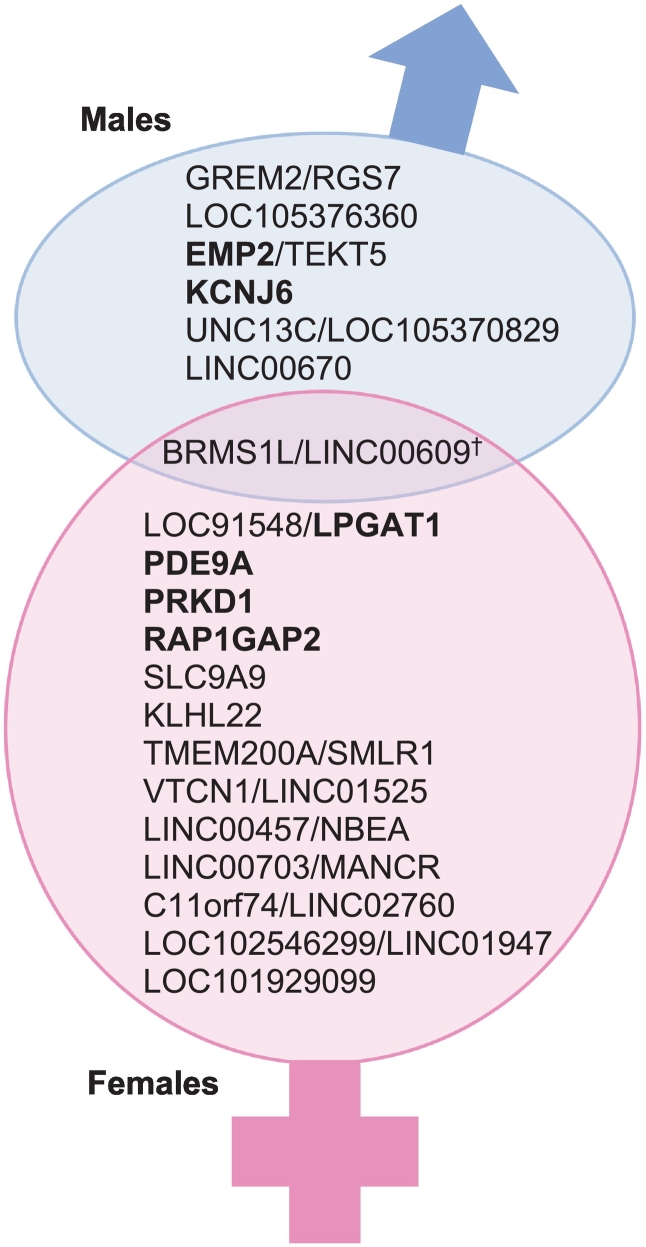
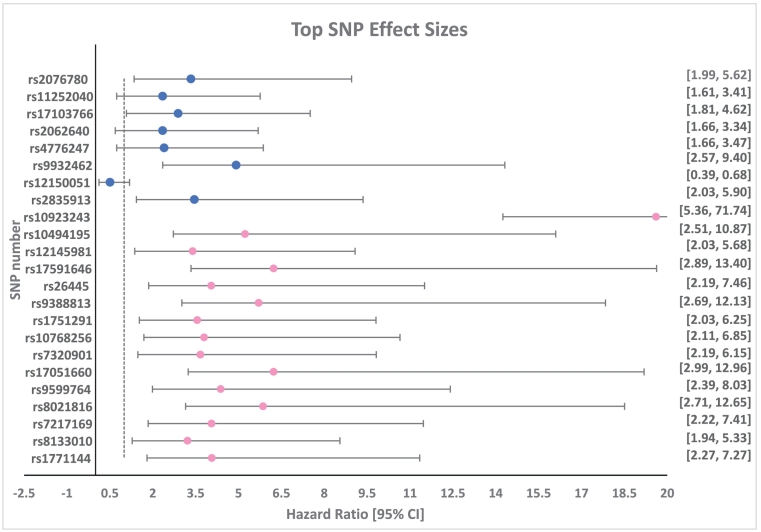
Results: The top GWAS hits associated with all-cause mortality among people with CAD included 8 SNPs among males and 15 among females (p = 1 × 10-6 or 10-7), adjusted for covariates. Cross-sex comparisons revealed distinct candidate genes. Biologically relevant candidates included rs9932462 (EMP2/TEKT5) and rs2835913 (KCNJ6) among males and rs7217169 (RAP1GAP2), rs8021816 (PRKD1), rs8133010 (PDE9A), and rs12145981 (LPGAT1) among females.
Conclusions: We report 20 sex-specific candidate genes having suggestive association with all-cause mortality among CAD-diagnosed subjects. Findings demonstrate proof of principle for identifying sex-associated genetic factors that may help explain differential mortality risk in people with CAD. Replication and meta-analyses in larger studies with more diverse samples will strengthen future work in this area.
Keywords: Coronary artery disease; Genome-wide association study; Sex differences; Sex dimorphism; Survival analysis.
Conflict of interest statement
Declaration of competing interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Genome-Wide Variants Associated With Longitudinal Survival Outcomes Among Individuals With Coronary Artery Disease.Front Genet. 2021 Jun 1;12:661497. doi: 10.3389/fgene.2021.661497. eCollection 2021. Front Genet. 2021. PMID: 34140969 Free PMC article.
-
Case-Only Survival Analysis Reveals Unique Effects of Genotype, Sex, and Coronary Disease Severity on Survivorship.PLoS One. 2016 May 17;11(5):e0154856. doi: 10.1371/journal.pone.0154856. eCollection 2016. PLoS One. 2016. PMID: 27187494 Free PMC article.
-
Exploring associations between estrogen and gene candidates identified by coronary artery disease genome-wide association studies.Front Cardiovasc Med. 2025 Mar 20;12:1502985. doi: 10.3389/fcvm.2025.1502985. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40182431 Free PMC article.
-
Exploring sex-specific genetic architecture of coronary artery disease in Tehran: a cardiometabolic genetic study.Expert Rev Mol Diagn. 2024 Dec 5:1-10. doi: 10.1080/14737159.2024.2436399. Online ahead of print. Expert Rev Mol Diagn. 2024. PMID: 39639470
-
Genome-Wide Association Studies and Risk Scores for Coronary Artery Disease: Sex Biases.Adv Exp Med Biol. 2018;1065:627-642. doi: 10.1007/978-3-319-77932-4_38. Adv Exp Med Biol. 2018. PMID: 30051411 Review.
Cited by
-
Brief biology and pathophysiology of Tekt bundles.Cell Adh Migr. 2025 Dec;19(1):2465421. doi: 10.1080/19336918.2025.2465421. Epub 2025 Feb 13. Cell Adh Migr. 2025. PMID: 39949046 Free PMC article. Review.
-
Research summary of poster presentations at the 2023 Florida cardio-oncology symposium.Am Heart J Plus. 2023 Nov 25;37:100348. doi: 10.1016/j.ahjo.2023.100348. eCollection 2024 Jan. Am Heart J Plus. 2023. PMID: 38510509 Free PMC article. No abstract available.
References
-
- Virani S.S., et al. Heart disease and stroke statistics—2020 update: a report from the American Heart Association. Circulation. 2020:E139–E596. - PubMed
-
- Izadnegahdar M., et al. Sex and ethnic differences in outcomes of acute coronary syndrome and stable angina patients with obstructive coronary artery disease. Circ. Cardiovasc. Qual. Outcomes. 2016;9(2 Suppl 1):S26–S35. - PubMed
-
- Chandrasekhar J., Mehran R. Sex-based differences in acute coronary syndromes: insights from invasive and noninvasive coronary technologies. JACC Cardiovasc. Imaging. 2016;9(4):451–464. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
