

Prediction of acute kidney injury in patients with femoral neck fracture utilizing machine learning
- PMID: 35959132
- PMCID: PMC9360500
- DOI: 10.3389/fsurg.2022.928750
Prediction of acute kidney injury in patients with femoral neck fracture utilizing machine learning
Abstract
Background: Acute kidney injury (AKI) is a common complication associated with significant morbidity and mortality in high-energy trauma patients. Given the poor efficacy of interventions after AKI development, it is important to predict AKI before its diagnosis. Therefore, this study aimed to develop models using machine learning algorithms to predict the risk of AKI in patients with femoral neck fractures.
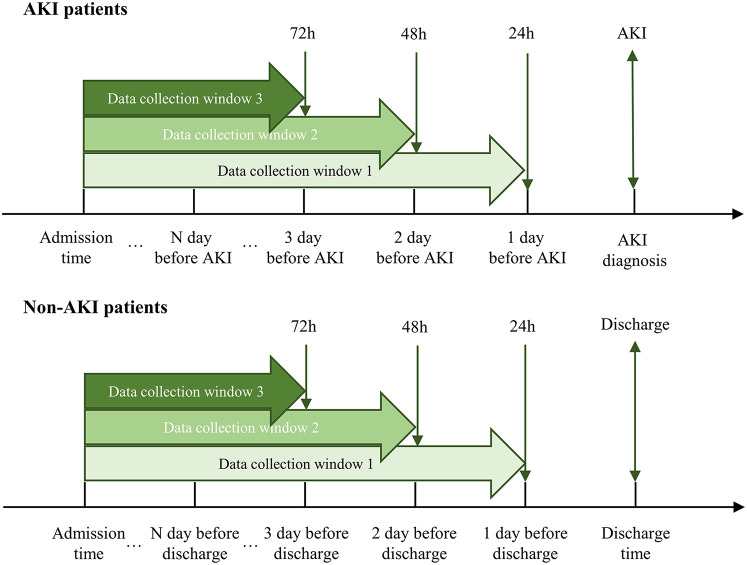
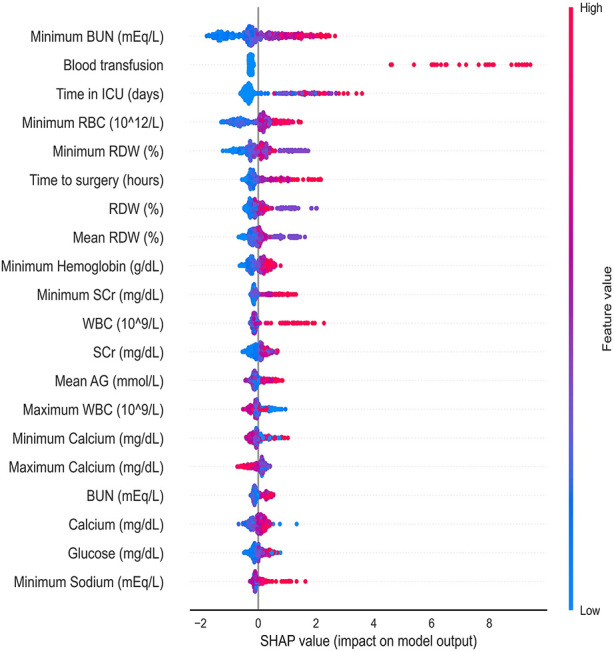
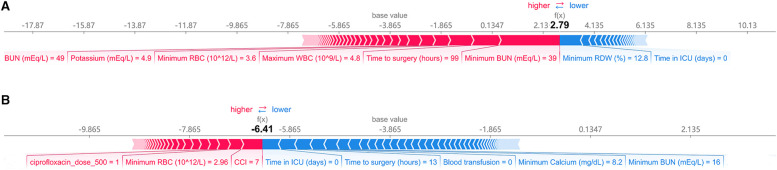
Methods: We developed machine-learning models using the Medical Information Mart from Intensive Care (MIMIC)-IV database. AKI was predicted using 10 predictive models in three-time windows, 24, 48, and 72 h. Three optimal models were selected according to the accuracy and area under the receiver operating characteristic curve (AUROC), and the hyperparameters were adjusted using a random search algorithm. The Shapley additive explanation (SHAP) analysis was used to determine the impact and importance of each feature on the prediction. Compact models were developed using important features chosen based on their SHAP values and clinical availability. Finally, we evaluated the models using metrics such as accuracy, precision, AUROC, recall, F1 scores, and kappa values on the test set after hyperparameter tuning.
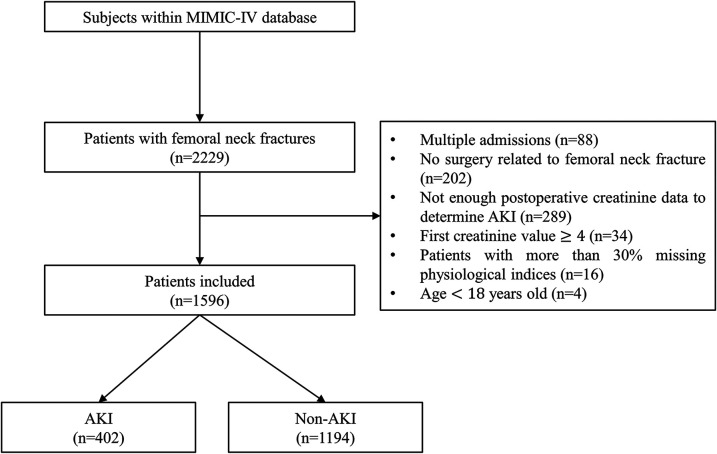
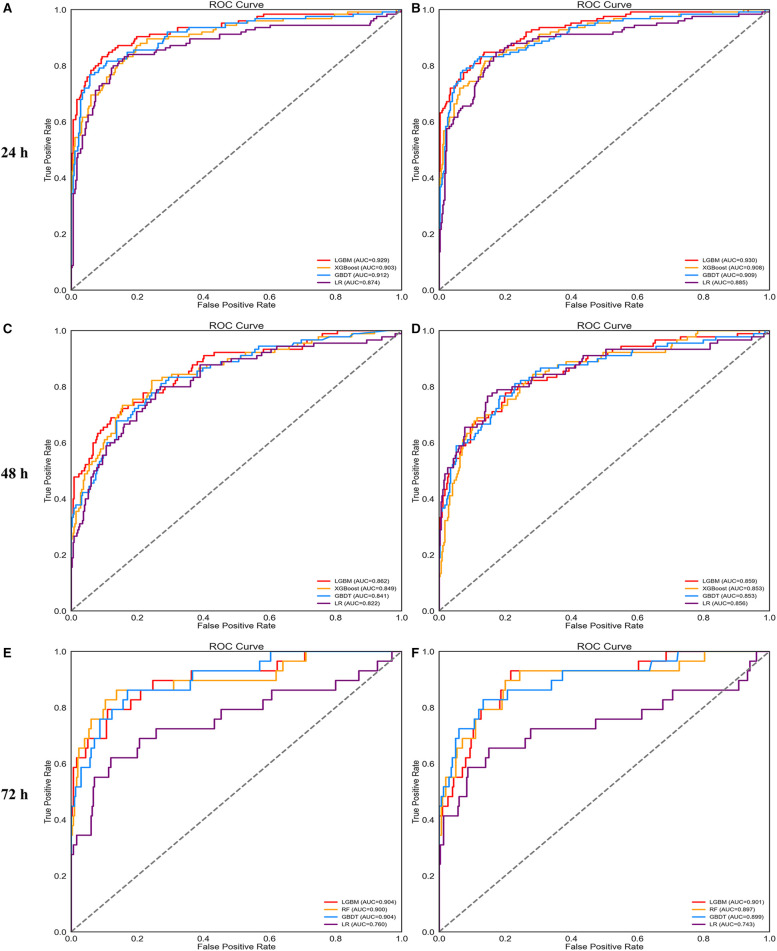
Results: A total of 1,596 patients in MIMIC-IV were included in the final cohort, and 402 (25%) patients developed AKI after surgery. The light gradient boosting machine (LightGBM) model showed the best overall performance for predicting AKI before 24, 48, and 72 h. AUROCs were 0.929, 0.862, and 0.904. The SHAP value was used to interpret the prediction models. Renal function markers and perioperative blood transfusions are the most critical features for predicting AKI. In compact models, LightGBM still performs the best. AUROCs were 0.930, 0.859, and 0.901.
Conclusions: In our analysis, we discovered that LightGBM had the best metrics among all algorithms used. Our study identified the LightGBM as a solid first-choice algorithm for early AKI prediction in patients after femoral neck fracture surgery.
Keywords: MIMIC-IV database; acute kidney injury; femoral neck fracture; machine learning; model interpretation; postoperative.
© 2022 Liu, Xu, Zhu, Han and Ai.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
A Machine Learning-Based Prediction Model for Acute Kidney Injury in Patients With Congestive Heart Failure.Front Cardiovasc Med. 2022 Mar 4;9:842873. doi: 10.3389/fcvm.2022.842873. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35310995 Free PMC article.
-
Predicting acute kidney injury risk in acute myocardial infarction patients: An artificial intelligence model using medical information mart for intensive care databases.Front Cardiovasc Med. 2022 Sep 7;9:964894. doi: 10.3389/fcvm.2022.964894. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36158815 Free PMC article.
-
Machine learning-based prediction model of acute kidney injury in patients with acute respiratory distress syndrome.BMC Pulm Med. 2023 Oct 3;23(1):370. doi: 10.1186/s12890-023-02663-6. BMC Pulm Med. 2023. PMID: 37789305 Free PMC article.
-
Predicting renal function recovery and short-term reversibility among acute kidney injury patients in the ICU: comparison of machine learning methods and conventional regression.Ren Fail. 2022 Dec;44(1):1326-1337. doi: 10.1080/0886022X.2022.2107542. Ren Fail. 2022. PMID: 35930309 Free PMC article. Review.
-
Acute Kidney Injury Prognosis Prediction Using Machine Learning Methods: A Systematic Review.Kidney Med. 2024 Nov 15;7(1):100936. doi: 10.1016/j.xkme.2024.100936. eCollection 2025 Jan. Kidney Med. 2024. PMID: 39758155 Free PMC article. Review.
Cited by
-
Differentiation Between Phyllodes Tumor and Fibroadenoma of the Breast: A Radiomics Prediction Model Based on Full-Field Digital Mammography & Digital Tomosynthesis.Technol Cancer Res Treat. 2024 Jan-Dec;23:15330338241289474. doi: 10.1177/15330338241289474. Technol Cancer Res Treat. 2024. PMID: 39376181 Free PMC article.
-
Exploring the role of Artificial Intelligence in Acute Kidney Injury management: a comprehensive review and future research agenda.BMC Med Inform Decis Mak. 2024 Nov 14;24(1):337. doi: 10.1186/s12911-024-02758-y. BMC Med Inform Decis Mak. 2024. PMID: 39543611 Free PMC article.
-
Systematic review of machine-learning models in orthopaedic trauma.Bone Jt Open. 2024 Jan 16;5(1):9-19. doi: 10.1302/2633-1462.51.BJO-2023-0095.R1. Bone Jt Open. 2024. PMID: 38226447 Free PMC article.
-
Automatic Feature Selection for Imbalanced Echocardiogram Data Using Event-Based Self-Similarity.Diagnostics (Basel). 2025 Apr 11;15(8):976. doi: 10.3390/diagnostics15080976. Diagnostics (Basel). 2025. PMID: 40310367 Free PMC article.
-
Comorbidities, acute kidney injury and long-term mortality in elderly patients hospitalized because of hip fracture: a moderation analysis.Aging Clin Exp Res. 2024 May 30;36(1):123. doi: 10.1007/s40520-024-02771-1. Aging Clin Exp Res. 2024. PMID: 38811522 Free PMC article.
References
LinkOut - more resources
Full Text Sources