

Perioperative Management and Surgical Outcomes of Colorectal Cancer Patients Undergoing Peritoneal Dialysis for End-Stage Kidney Disease
- PMID: 35959175
- PMCID: PMC9360629
- DOI: 10.7759/cureus.26708
Perioperative Management and Surgical Outcomes of Colorectal Cancer Patients Undergoing Peritoneal Dialysis for End-Stage Kidney Disease
Abstract
Introduction: Despite the fact that the number of peritoneal dialysis (PD) patients is increasing, there is little evidence on the surgical outcomes of PD patients who have colorectal cancer surgery, and there is no consensus on the safety and practicality of continuing PD.
Methods: We retrospectively evaluated the short- and long-term results, as well as the feasibility of continuing PD, in eight patients with PD who had colorectal cancer surgery at our institution between January 2010 and January 2021.
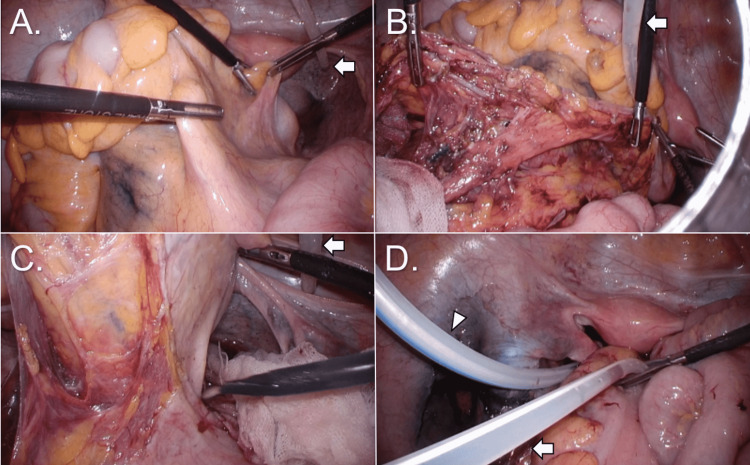
Results: The scheduled open-fashioned resection was performed in one patient, whereas the other seven surgeries were all conducted laparoscopically, with no intraoperative conversion to laparotomy necessary. Except for one patient with a history of recurring PD-related peritonitis, the PD catheter was kept in seven of the eight cases. Five of the seven patients continuing PD underwent temporary postoperative hemodialysis. At a median of 24.5 months of postoperative monitoring, no infectious complications were observed, six cases continued PD, and no recurrence of colorectal cancer was observed in all cases.
Conclusions: Routine curative-intent colorectal cancer surgery with the preservation of the PD catheter is possible and safe in individuals receiving PD. This patient population's short- and long-term oncological results are comparable to general surgical outcomes of those without chronic kidney disease. PD can be maintained for a long period of time following major colorectal cancer surgery.
Keywords: colorectal cancer surgery; end-stage kidney disease; end-stage renal disease; perioperative management; peritoneal dialysis; surgical outcome.
Copyright © 2022, Kouno et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Outcome and complications in peritoneal dialysis patients: a five-year single center experience.Saudi J Kidney Dis Transpl. 2011 Mar;22(2):245-51. Saudi J Kidney Dis Transpl. 2011. PMID: 21422621
-
Laparoscopic Left Hemicolectomy for Colon Cancer in Peritoneal Dialysis Patients: A Valid and Safe Surgical Technique to Ensure Peritoneal Dialysis Survival.Perit Dial Int. 2016 11-12;36(6):695-699. doi: 10.3747/pdi.2015.00259. Perit Dial Int. 2016. PMID: 27903856 Free PMC article.
-
Surgical Complications of Peritoneal Dialysis.Chirurgia (Bucur). 2018 Sept-Oct;113(5):611-624. doi: 10.21614/chirurgia.113.5.611. Chirurgia (Bucur). 2018. PMID: 30383988
-
The "Half-Perc" technique using a simple modified metal trocar for peritoneal dialysis catheter placement: results of a 3-year follow-up of 280 patients and a literature review.Int Urol Nephrol. 2022 Jul;54(7):1741-1749. doi: 10.1007/s11255-021-03028-w. Epub 2021 Nov 23. Int Urol Nephrol. 2022. PMID: 34813024 Review.
-
When end-stage kidney disease complicates abdominal surgery.Semin Dial. 2020 May;33(3):270-278. doi: 10.1111/sdi.12872. Epub 2020 Apr 10. Semin Dial. 2020. PMID: 32277515 Review.
References
-
- 2018 annual dialysis data report, JSDT Renal Data Registry. Nitta K, Masakane I, Hanafusa N, et al. Nihon Toseki Igakkai Zasshi. 2019;52:679–754.
-
- Continuous ambulatory peritoneal dialysis and the heart. Alpert MA, Hüting J, Twardowski ZJ, Khanna R, Nolph KD. Perit Dial Int. 1995;15:6–11. - PubMed
-
- Improving outcome in geriatric peritoneal dialysis patients. Hiramatsu M. Perit Dial Int. 2003;23:84–89. - PubMed
LinkOut - more resources
Full Text Sources