

Retroform Cervical Dystonia: Target Muscle Selection and Efficacy of Botulinum Toxin Injection
- PMID: 35959387
- PMCID: PMC9360915
- DOI: 10.3389/fneur.2022.952456
Retroform Cervical Dystonia: Target Muscle Selection and Efficacy of Botulinum Toxin Injection
Abstract
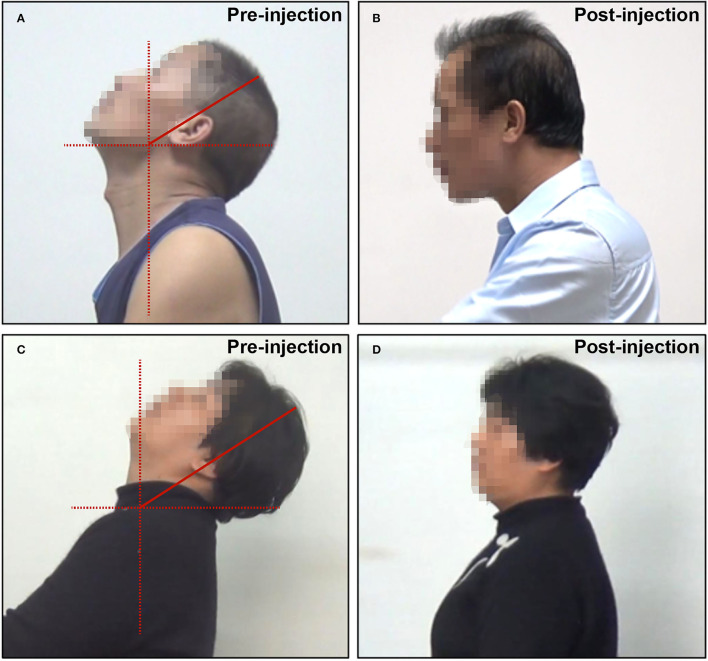
Introduction: Retroform cervical dystonia (RCD), which includes retrocaput and retrocollis, is a rare form of cervical dystonia. Few reports have been published on RCD. The present study aimed to characterize the target muscles involved in RCD and the efficacy of botulinum toxin type A (BTX-A) injection.
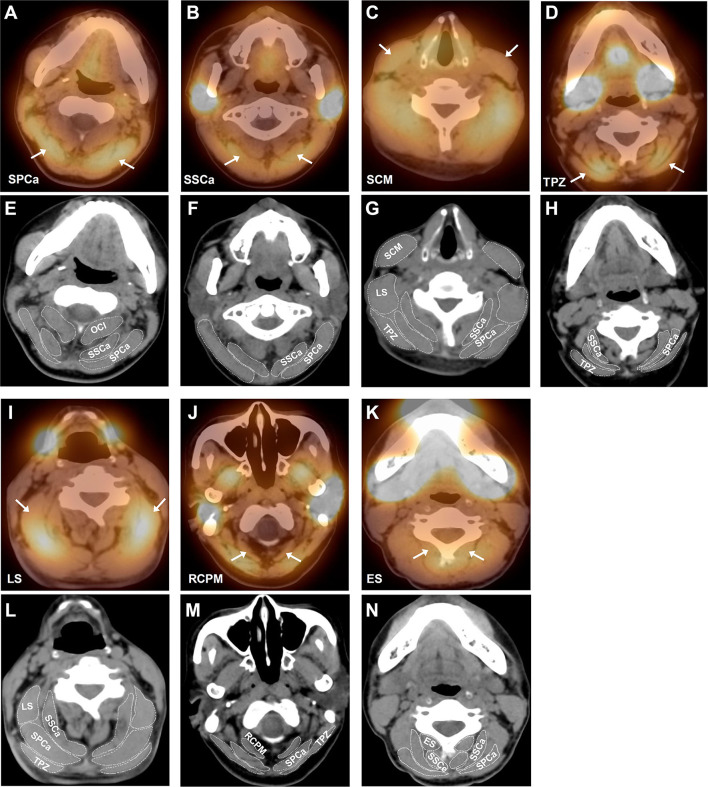
Methods: Patients with consecutive cervical dystonia with RCD as the most problematic feature were retrospectively analyzed over a 10-year period. Target muscles were screened and confirmed based on clinical evaluation, single-photon emission computed tomography, and electromyography. In addition, efficacy and adverse events following BTX-A injection in patients with RCD were evaluated.
Results: A total of 34 patients with RCD were included, 18 of whom presented with retrocaput and 16 with retrocollis. The most frequently injected muscles in RCD were splenius capitis (SPCa, 97.1%) and semispinalis capitis (SSCa, 97.1%), followed by levator scapulae (LS, 50.0%), rectus capitis posterior major (RCPM, 47.1%), trapezius (TPZ, 41.2%), and sternocleidomastoid muscle (SCM, 41.2%). Besides cervical muscles, the erector spinae was also injected in 17.6% of patients. Most muscles were predominantly bilaterally injected. The injection schemes of retrocaput and retrocollis were similar, possibly because in patients with retrocollis, retrocaput was often combined. BTX-A injection achieved a satisfactory therapeutic effect in RCD, with an average symptom relief rate of 69.0 ± 16.7%. Mild dysphagia (17.6%) and posterior cervical muscle weakness (17.6%) were the most common adverse events.
Conclusion: SPCa, SSCa, LS, RCPM, LS, and SCM were commonly and often bilaterally injected in RCD. Patients with RCD could achieve satisfactory symptom relief after BTX-A injection.
Keywords: botulinum toxin; cervical dystonia; retrocaput; retrocollis; single-photon emission computed tomography.
Copyright © 2022 Hu, Pan, Su, Chen, Zhang, Pan, Jin and Teng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Cervical dystonia: Injecting botulinum neurotoxin into semispinalis capitis improves goose-neck posture.Clin Park Relat Disord. 2019 Jul 15;1:8-9. doi: 10.1016/j.prdoa.2019.06.002. eCollection 2019. Clin Park Relat Disord. 2019. PMID: 34316591 Free PMC article.
-
Frequency of different subtypes of cervical dystonia: a prospective multicenter study according to Col-Cap concept.J Neural Transm (Vienna). 2020 Jan;127(1):45-50. doi: 10.1007/s00702-019-02116-7. Epub 2019 Dec 11. J Neural Transm (Vienna). 2020. PMID: 31828512
-
Accuracy of Ultrasound-Guided and Non-guided Botulinum Toxin Injection Into Neck Muscles Involved in Cervical Dystonia: A Cadaveric Study.Ann Rehabil Med. 2020 Oct;44(5):370-377. doi: 10.5535/arm.19211. Epub 2020 Sep 28. Ann Rehabil Med. 2020. PMID: 32986942 Free PMC article.
-
[Aspects of the complexity of cervical dystonia].Nervenarzt. 2008 Jun;79 Suppl 1:15-8. Nervenarzt. 2008. PMID: 18927959 Review. German.
-
Botulinum toxin B: a review of its therapeutic potential in the management of cervical dystonia.Drugs. 2002;62(4):705-22. doi: 10.2165/00003495-200262040-00011. Drugs. 2002. PMID: 11893235 Review.
References
LinkOut - more resources
Full Text Sources