

The influence of site on the incidence and diagnosis of solitary central cartilage tumours of the femur. A 21st century perspective
- PMID: 35959501
- PMCID: PMC9358228
- DOI: 10.1016/j.jcot.2022.101953
The influence of site on the incidence and diagnosis of solitary central cartilage tumours of the femur. A 21st century perspective
Abstract
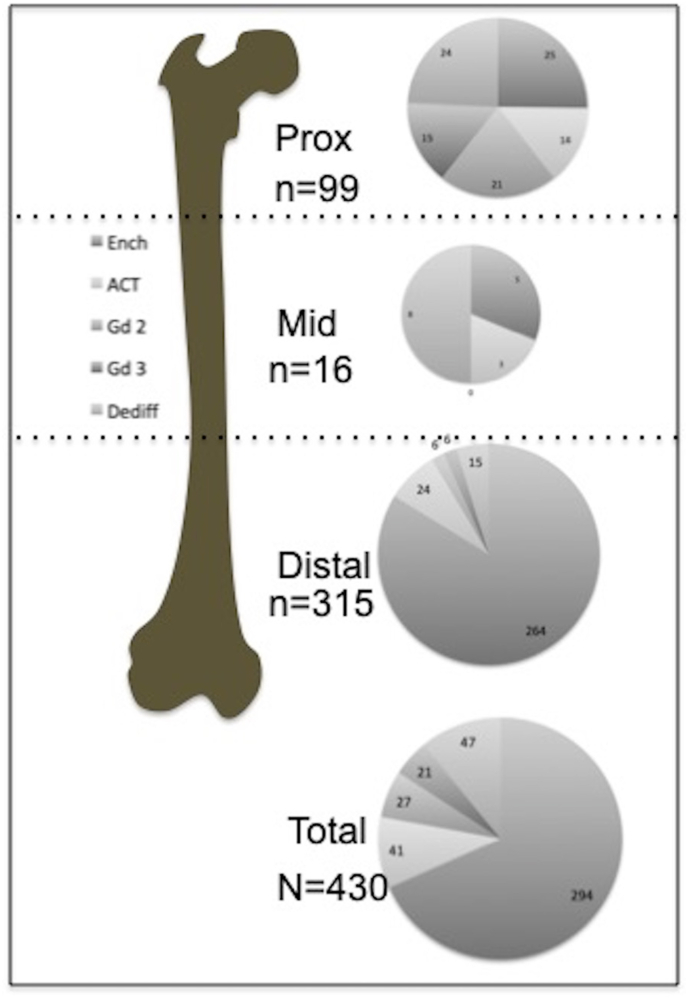
Objective: To determine the incidence of central cartilage tumours (CCTs) in the femur and the impact of site (proximal, mid and distal thirds) on tumour grade. To compare study results with historically published data.
Materials and methods: Retrospective review of solitary CCTs arising in the femur over the past 13 years. Data collected included location (proximal, mid and distal thirds) and final diagnosis in terms of tumour grade based on imaging features ± histology. Case material collected from three bone tumour textbooks provided historical data.
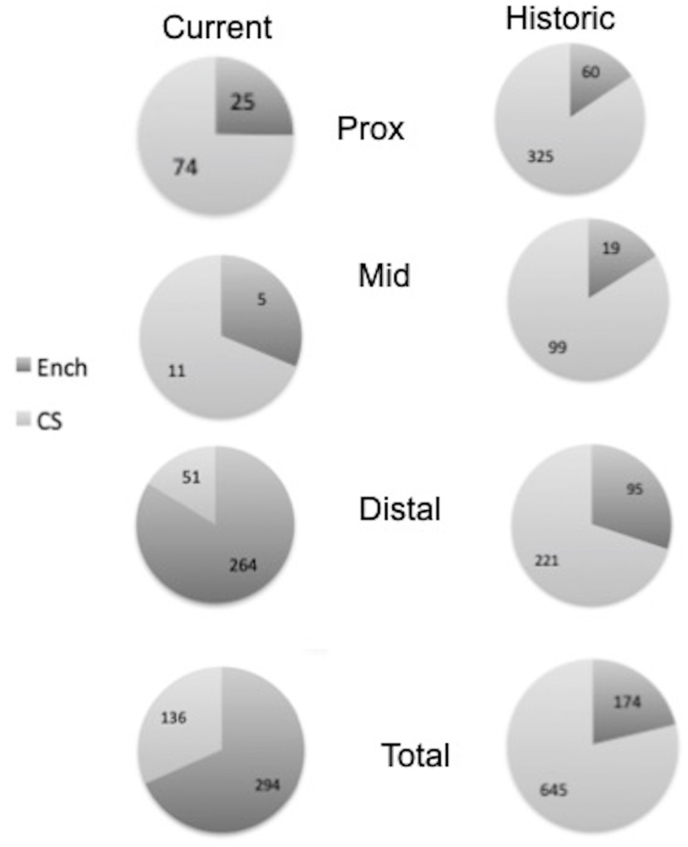
Results: 430 solitary CCTs were included in the femur. 73% cases arose in the distal, 3.7% in the mid and 23% in the proximal femur. The ratio of "benign" (combining enchondroma and atypical cartilaginous tumour (ACT)) to higher grade chondrosarcoma (CS) was 11:1 in the distal, 1:1 in the mid and 1:1.5 in the proximal femur, the distribution of benign to malignant tumours being significantly different between the regions (F test, p < 0.05). Comparison with historical data showed a reversal of the benign (enchondroma) to malignant (ACT and higher grade CS) of 30%:70%-84%:16% in the current series.
Conclusions: The site of origin of a CCT in the femur has an impact on final diagnosis with CS uncommon in the distal as compared with the mid and proximal femur. This is in contradistinction to historical data where the incidence of CS exceeded that of enchondroma at all sites.
Keywords: Central cartilage tumour; Femur; Solitary.
© 2022 Delhi Orthopedic Association. All rights reserved.
Conflict of interest statement
No conflicts of interest.
Figures
Similar articles
-
A retrospective external validation study of the Birmingham Atypical Cartilage Tumour Imaging Protocol (BACTIP) for the management of solitary central cartilage tumours of the proximal humerus and around the knee.Eur Radiol. 2024 Aug;34(8):4988-5006. doi: 10.1007/s00330-024-10604-y. Epub 2024 Feb 6. Eur Radiol. 2024. PMID: 38319428
-
A retrospective validation of an imaging protocol for the management of solitary central cartilage tumours of the proximal humerus and around the knee.Clin Radiol. 2019 Dec;74(12):962-971. doi: 10.1016/j.crad.2019.08.017. Epub 2019 Oct 3. Clin Radiol. 2019. PMID: 31587800
-
An imaging protocol for the management of central cartilage tumours of the proximal fibula.Clin Radiol. 2020 Sep;75(9):714.e1-714.e6. doi: 10.1016/j.crad.2020.03.040. Epub 2020 Jul 11. Clin Radiol. 2020. PMID: 32665062
-
Co-existence of lung carcinoma metastasis and enchondroma in the femur of a patient with Ollier disease.Virchows Arch. 2021 Jul;479(1):203-207. doi: 10.1007/s00428-020-02936-z. Epub 2020 Oct 13. Virchows Arch. 2021. PMID: 33047157 Free PMC article. Review.
-
A pragmatic approach to the imaging and follow-up of solitary central cartilage tumours of the proximal humerus and knee.Clin Radiol. 2019 Jul;74(7):517-526. doi: 10.1016/j.crad.2019.01.025. Epub 2019 Mar 1. Clin Radiol. 2019. PMID: 30827492 Review.
Cited by
-
Chondrosarcoma of the Femur: Is Local Recurrence Influenced by the Presence of an Extraosseous Component?Cancers (Basel). 2024 Jan 15;16(2):363. doi: 10.3390/cancers16020363. Cancers (Basel). 2024. PMID: 38254852 Free PMC article.
References
-
- Brien E.W., Mirra J.M., Kerr R. Benign and malignant cartilage tumors of bone and joint: their anatomic and theoretical basis with an emphasis on radiology, pathology and clinical biology. 1. The intramedullary tumors. Skeletal Radiol. 1997;26:325–353. - PubMed
-
- Suster D., Hung Y.P., Nielsen G.P. Differential diagnosis of cartilaginous lesions of bone. Arch Pathol Lab Med. 2020;144:71–82. - PubMed
-
- Davies A.M., Shah A., Shah R., Patel A., James S.L., Botchu R. Are the tubular bones of the hand really the commonest site for an enchondroma? Clin Radiol. 2020;75:533–537. - PubMed
-
- Walden M.J., Murphey M.D., Vidal J.A. Incidental enchondromas of the knee. AJR Am J Roentgenol. 2008;190:1611–1615. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous