

Pembrolizumab, radiotherapy, and an immunomodulatory five-drug cocktail in pretreated patients with persistent, recurrent, or metastatic cervical or endometrial carcinoma: Results of the phase II PRIMMO study
- PMID: 35960332
- PMCID: PMC9870976
- DOI: 10.1007/s00262-022-03253-x
Pembrolizumab, radiotherapy, and an immunomodulatory five-drug cocktail in pretreated patients with persistent, recurrent, or metastatic cervical or endometrial carcinoma: Results of the phase II PRIMMO study
Erratum in
-
Correction: Pembrolizumab, radiotherapy, and an immunomodulatory five-drug cocktail in pretreated patients with persistent, recurrent, or metastatic cervical or endometrial carcinoma: Results of the phase II PRIMMO study.Cancer Immunol Immunother. 2024 Dec 30;74(1):32. doi: 10.1007/s00262-024-03873-5. Cancer Immunol Immunother. 2024. PMID: 39738642 Free PMC article. No abstract available.
Abstract
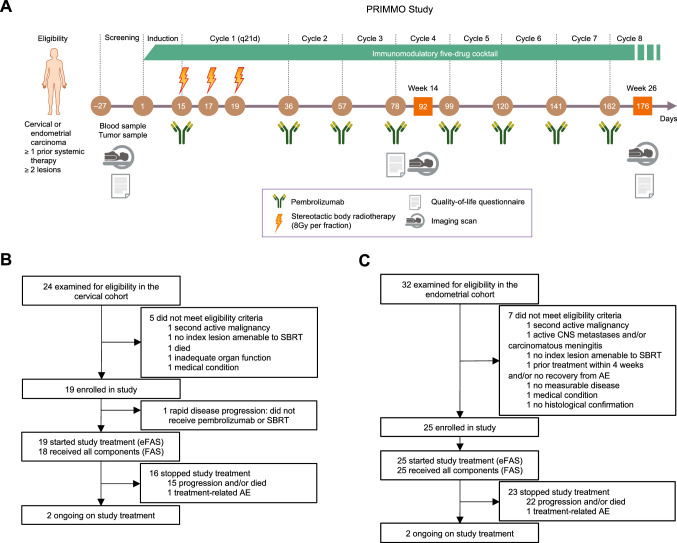
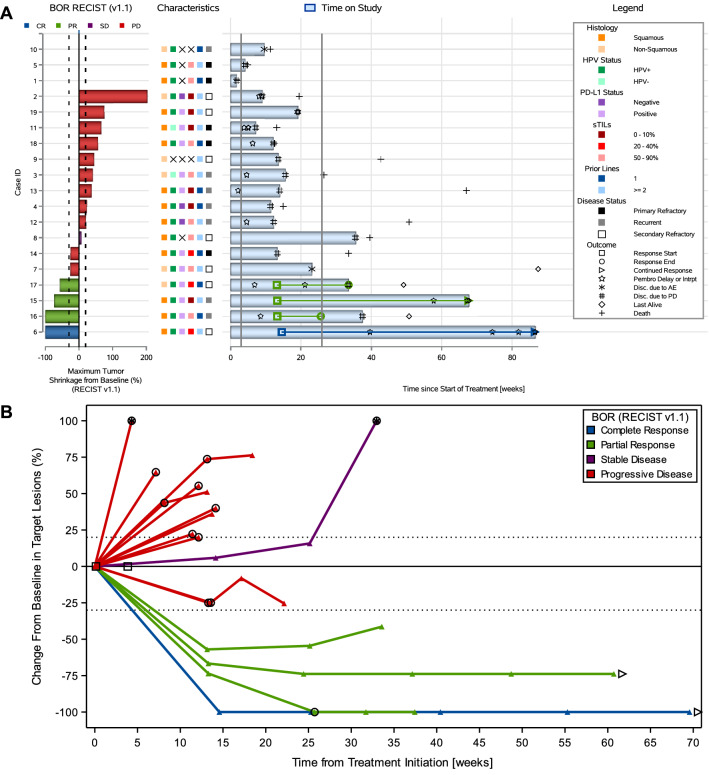
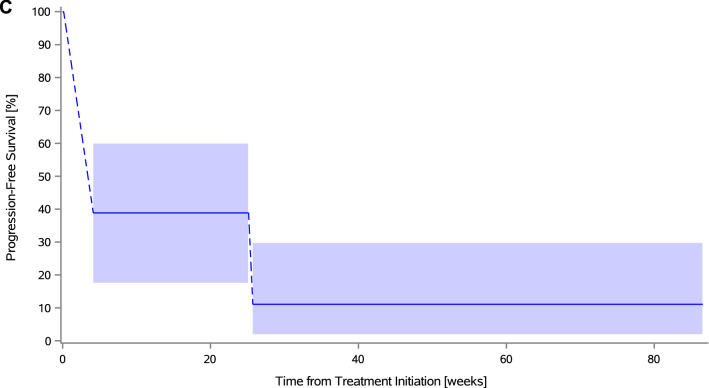
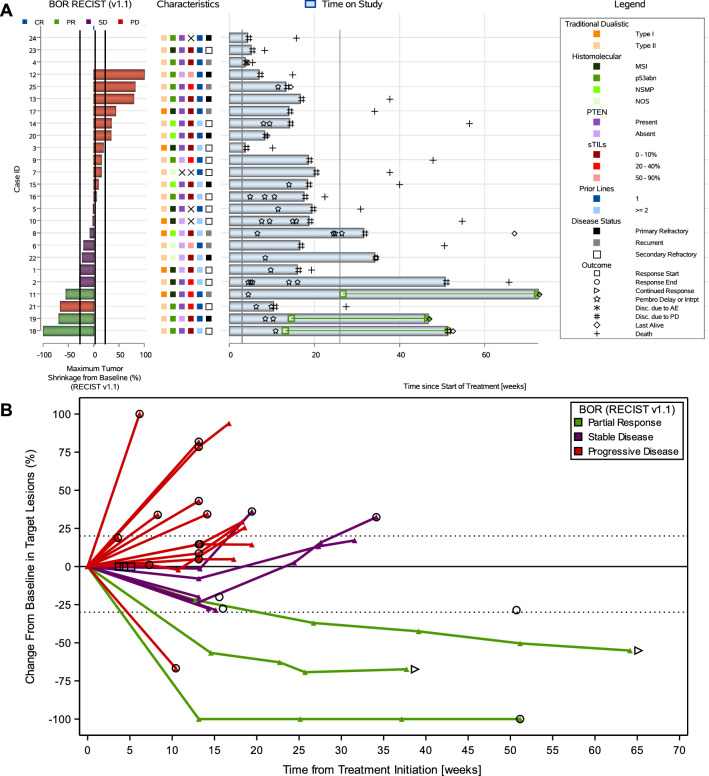
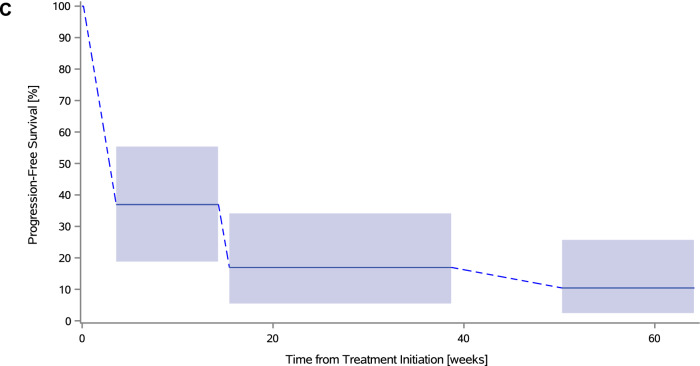
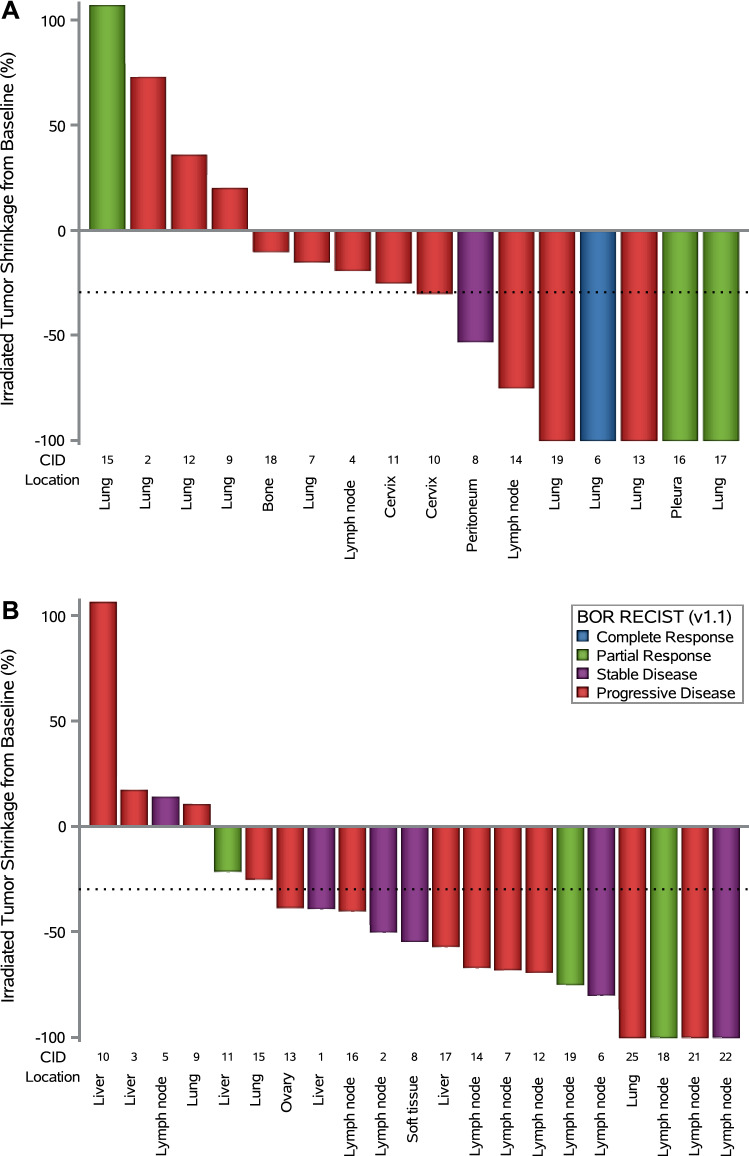
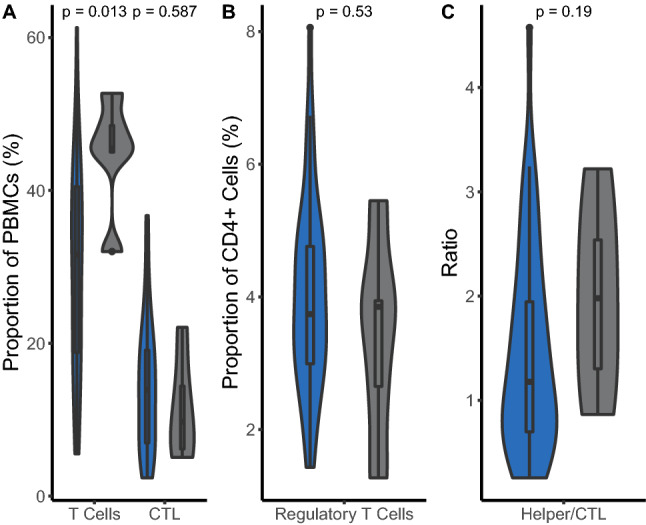
A phase II study (PRIMMO) of patients with pretreated persistent/recurrent/metastatic cervical or endometrial cancer is presented. Patients received an immunomodulatory five-drug cocktail (IDC) consisting of low-dose cyclophosphamide, aspirin, lansoprazole, vitamin D, and curcumin starting 2 weeks before radioimmunotherapy. Pembrolizumab was administered three-weekly from day 15 onwards; one of the tumor lesions was irradiated (8Gyx3) on days 15, 17, and 19. The primary endpoint was the objective response rate per immune-related response criteria (irORR) at week 26 (a lower bound of the 90% confidence interval [CI] of > 10% was considered efficacious). The prespecified 43 patients (cervical, n = 18; endometrial, n = 25) were enrolled. The irORR was 11.1% (90% CI 2.0-31.0) in cervical cancer and 12.0% (90% CI 3.4-28.2) in endometrial cancer. Median duration of response was not reached in both cohorts. Median interval-censored progression-free survival was 4.1 weeks (95% CI 4.1-25.7) in cervical cancer and 3.6 weeks (95% CI 3.6-15.4) in endometrial cancer; median overall survival was 39.6 weeks (95% CI 15.0-67.0) and 37.4 weeks (95% CI 19.0-50.3), respectively. Grade ≥ 3 treatment-related adverse events were reported in 10 (55.6%) cervical cancer patients and 9 (36.0%) endometrial cancer patients. Health-related quality of life was generally stable over time. Responders had a significantly higher proportion of peripheral T cells when compared to nonresponders (p = 0.013). In conclusion, PRIMMO did not meet its primary objective in both cohorts; pembrolizumab, radiotherapy, and an IDC had modest but durable antitumor activity with acceptable but not negligible toxicity.Trial registration ClinicalTrials.gov (identifier NCT03192059) and EudraCT Registry (number 2016-001569-97).
Keywords: Drug therapy, combination; Gynecologic neoplasms; Immunomodulation; Radioimmunotherapy; Tumor microenvironment.
© 2022. The Author(s).
Conflict of interest statement
EAD: travel and accommodation expenses (institutional, not personal) from AstraZeneca, GSK, Pfizer, and PharmaMar. AMTV: became an employee for GSK during the publication development. PV: consulting or advisory role (personal) from Eli Lily and Company, MSD, Mundipharma, Novartis, Pfizer, and Roche; research funding from Tesaro. SH: consulting or advisory role (personal) from AstraZeneca, BMSi, Gilead Sciences, Merck, MSD Oncology, Novartis, and Sanofi. SA: consulting or advisory role (institutional, not personal) for MSD, Sanofi, Roche, BMS, and Pfizer; research funding (institutional, not personal) from Sanofi. AD: research funding (institutional, not personal) from AstraZeneca. EN: travel and accommodation expenses (institutional, not personal) from AstraZeneca, Novartis, Pfizer, PharmaMar, Roche, and Teva. DL: consulting or advisory role (institutional, not personal) for AstraZeneca, Biocartis, BMS, Boehringer Ingelheim, Eli Lilly and Company, Hedera Dx, Montis Biosciences, MSD; consulting or advisory role (personal) for AstraZeneca, Biocartis, Montis Biosciences, and MSD. FA: consulting or advisory role (institutional, not personal) for MiMark. KV: travel and accommodation expenses (institutional, not personal) from PharmaMar. HGD: travel and accommodation expenses (institutional, not personal) from Amgen, AstraZeneca, Eli Lily and Company, GSK, MSD, Novartis, Pfizer, PharmaMar, Roche, Tesaro, and Teva; research funding (institutional, not personal) from Roche. ST, AB, KB, RB, LL, XBT, PAV, AH, OD, and KKV: declare no competing interests.
Figures
Similar articles
-
PRIMMO study protocol: a phase II study combining PD-1 blockade, radiation and immunomodulation to tackle cervical and uterine cancer.BMC Cancer. 2019 May 28;19(1):506. doi: 10.1186/s12885-019-5676-3. BMC Cancer. 2019. PMID: 31138229 Free PMC article. Clinical Trial.
-
Associations of the gut microbiome with outcomes in cervical and endometrial cancer patients treated with pembrolizumab: Insights from the phase II PRIMMO trial.Gynecol Oncol. 2024 Dec;191:275-286. doi: 10.1016/j.ygyno.2024.10.020. Epub 2024 Nov 7. Gynecol Oncol. 2024. PMID: 39515198 Clinical Trial.
-
Health-related quality of life with pembrolizumab or placebo plus chemotherapy with or without bevacizumab for persistent, recurrent, or metastatic cervical cancer (KEYNOTE-826): a randomised, double-blind, placebo-controlled, phase 3 trial.Lancet Oncol. 2023 Apr;24(4):392-402. doi: 10.1016/S1470-2045(23)00052-9. Epub 2023 Mar 3. Lancet Oncol. 2023. PMID: 36878237 Clinical Trial.
-
Correction: Pembrolizumab, radiotherapy, and an immunomodulatory five-drug cocktail in pretreated patients with persistent, recurrent, or metastatic cervical or endometrial carcinoma: Results of the phase II PRIMMO study.Cancer Immunol Immunother. 2024 Dec 30;74(1):32. doi: 10.1007/s00262-024-03873-5. Cancer Immunol Immunother. 2024. PMID: 39738642 Free PMC article. No abstract available.
-
Lenvatinib plus pembrolizumab in patients with advanced endometrial cancer: an interim analysis of a multicentre, open-label, single-arm, phase 2 trial.Lancet Oncol. 2019 May;20(5):711-718. doi: 10.1016/S1470-2045(19)30020-8. Epub 2019 Mar 25. Lancet Oncol. 2019. PMID: 30922731 Free PMC article. Clinical Trial.
Cited by
-
First-in-human study of SBRT and adenosine pathway blockade to potentiate the benefit of immunochemotherapy in early-stage luminal B breast cancer: results of the safety run-in phase of the Neo-CheckRay trial.J Immunother Cancer. 2023 Dec 6;11(12):e007279. doi: 10.1136/jitc-2023-007279. J Immunother Cancer. 2023. PMID: 38056900 Free PMC article. Clinical Trial.
-
Platelets in cancer and immunotherapy: functional dynamics and therapeutic opportunities.Exp Hematol Oncol. 2025 Jun 13;14(1):83. doi: 10.1186/s40164-025-00676-x. Exp Hematol Oncol. 2025. PMID: 40514754 Free PMC article. Review.
-
Enhancing cancer immunotherapy using cordycepin and Cordyceps militaris extract to sensitize cancer cells and modulate immune responses.Sci Rep. 2024 Sep 19;14(1):21907. doi: 10.1038/s41598-024-72833-x. Sci Rep. 2024. PMID: 39300166 Free PMC article.
-
Role of the tumor microenvironment in the lymphatic metastasis of cervical cancer (Review).Exp Ther Med. 2023 Sep 1;26(4):486. doi: 10.3892/etm.2023.12185. eCollection 2023 Oct. Exp Ther Med. 2023. PMID: 37753293 Free PMC article. Review.
-
Advances and Challenges in the Treatment of HPV-Associated Lower Genital Tract Cancers by Immune Checkpoint Blockers: Insights from Basic and Clinical Science.Cancers (Basel). 2025 Apr 8;17(8):1260. doi: 10.3390/cancers17081260. Cancers (Basel). 2025. PMID: 40282436 Free PMC article. Review.
References
-
- McMeekin DS, Filiaci VL, Thigpen JT, Gallion HH, Fleming GF, Rodgers WH (2007) The relationship between histology and outcome in advanced and recurrent endometrial cancer patients participating in first-line chemotherapy trials: a Gynecologic Oncology Group study. Gynecol Oncol 106(1):16–22 - PubMed
-
- Tewari KS, Sill MW, Penson RT, Huang H, Ramondetta LM, Landrum LM et al (2017) Bevacizumab for advanced cervical cancer: final overall survival and adverse event analysis of a randomised, controlled, open-label, phase 3 trial (Gynecologic Oncology Group 240). Lancet 390(10103):1654–1663 - PMC - PubMed
-
- Concin N, Matias-Guiu X, Vergote I, Cibula D, Mirza MR, Marnitz S et al (2021) ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int J Gynecol Cancer 31(1):12–39 - PubMed
-
- Marth C, Landoni F, Mahner S, McCormack M, Gonzalez-Martin A, Colombo N (2017) Cervical cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol Off J Eur Soc Med Oncol 28(suppl_4):72–83 - PubMed
