

Bullous pemphigoid anti-BP180-NC16A autoantibody reactivity in healthy individuals is associated with marked hypovitaminosis D and Th2-like cytokine predominance
- PMID: 35960354
- PMCID: PMC10615949
- DOI: 10.1007/s00403-022-02386-4
Bullous pemphigoid anti-BP180-NC16A autoantibody reactivity in healthy individuals is associated with marked hypovitaminosis D and Th2-like cytokine predominance
Abstract
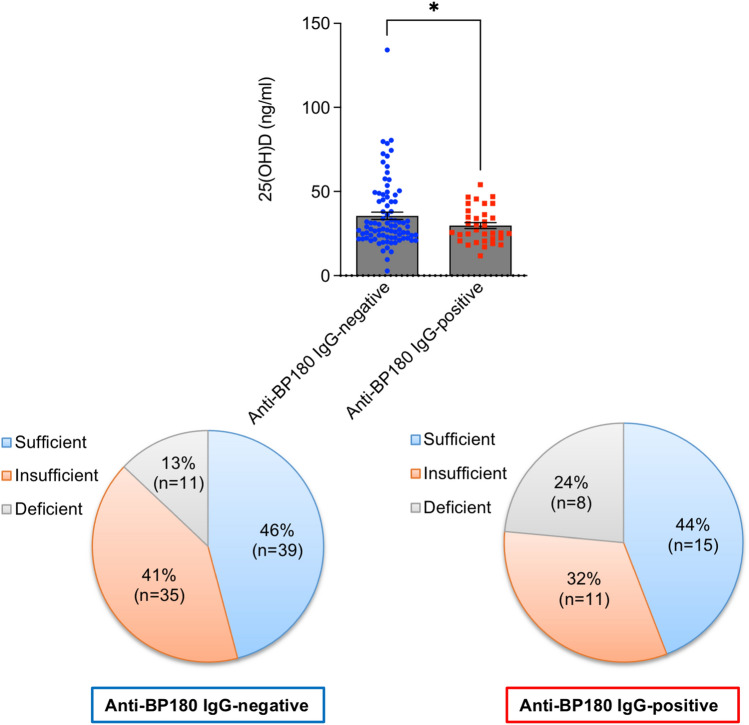
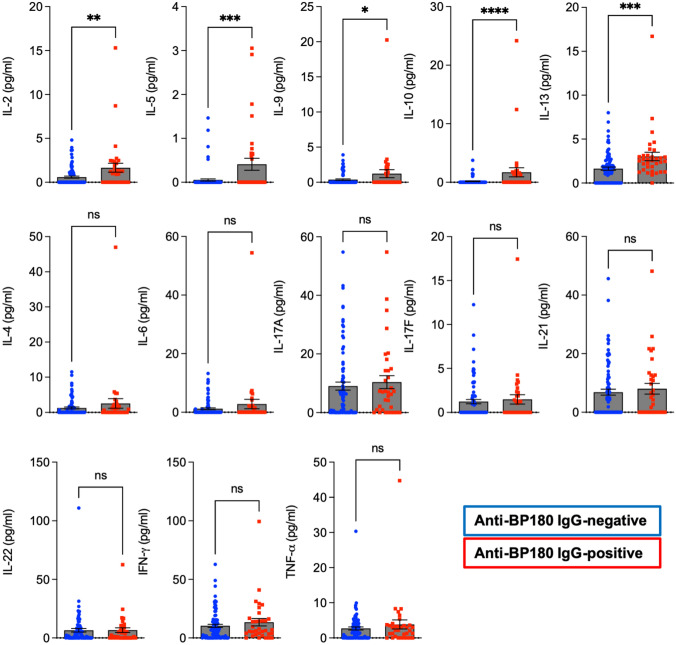
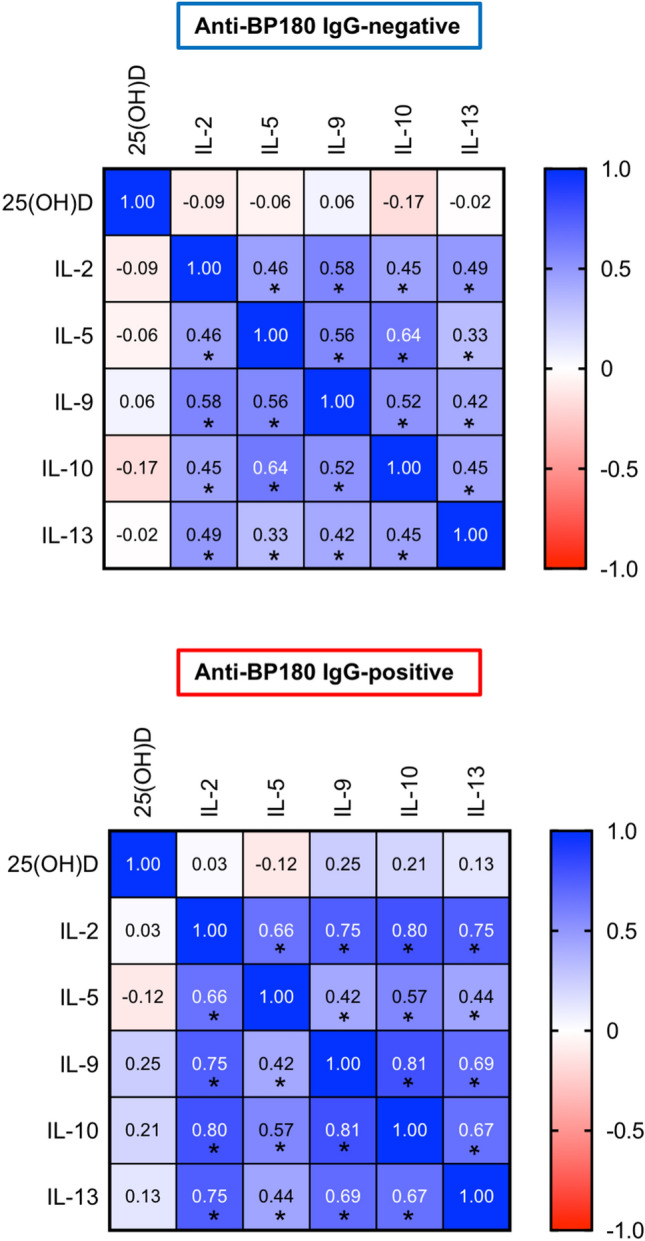
Autoimmune bullous disease autoantibodies, particularly including bullous pemphigoid (BP)-related anti-BP180-NC16A IgG, have been reported in a small subset of healthy individuals, but information about associated factors is lacking. We hypothesized that an abnormal status of immunomodulatory vitamin D could play a role in anti-BP180-NC16A autoantibody reactivity in healthy persons. In addition, we aimed to evaluate the cytokine profile associated with these autoantibodies. Plasma samples from 34 anti-BP180-NC16A IgG-reactive and 85 anti-BP180-NC16A IgG-negative healthy blood donors were tested for levels of 25-hydroxyvitamin D [25(OH)D] and a wide range of cytokines (IL-2, IL-4, IL-5, IL-6, IL-9, IL-10, IL-13, IL-17A, IL-17F, IL-21, IL-22, IFN-γ, and TNF-α). We observed that anti-BP180-NC16A IgG-reactive healthy subjects had significantly lower plasma 25(OH)D levels and about a two-fold higher rate of vitamin D deficiency (< 20 ng/ml) compared to anti-BP180-NC16A IgG-negative healthy persons. In addition, anti-BP180-NC16A IgG-positive samples were characterized by significantly higher levels of IL-2, IL-5, IL-9, IL-10, and IL-13 which were, however, not significantly associated with the vitamin D levels. Our results indicate that healthy individuals with BP autoantibody reactivity share similarities with BP patients regarding the vitamin D status and cytokine profile (i.e., marked hypovitaminosis D and Th2 predominance), which may have pathophysiologic implications.
Keywords: 25(OH)D; Bullous pemphigoid; Cytokine; Th2; Vitamin D.
© 2022. The Author(s).
Conflict of interest statement
There are no competing conflicts of interest.
Figures
Similar articles
-
IgE anti-BP180 NC16A autoantibody in both serum and blister fluid samples does not correlate with disease activity of bullous pemphigoid.Eur J Dermatol. 2023 Dec 1;33(6):595-603. doi: 10.1684/ejd.2023.4573. Eur J Dermatol. 2023. PMID: 38465539
-
Correlation of Serum Levels of IgE Autoantibodies Against BP180 With Bullous Pemphigoid Disease Activity.JAMA Dermatol. 2017 Jan 1;153(1):30-38. doi: 10.1001/jamadermatol.2016.3357. JAMA Dermatol. 2017. PMID: 27829102
-
Development of a novel ELISA system for detection of anti-BP180 IgG and characterization of autoantibody profile in bullous pemphigoid patients.Br J Dermatol. 2004 Nov;151(5):1004-10. doi: 10.1111/j.1365-2133.2004.06245.x. Br J Dermatol. 2004. PMID: 15541078
-
Bullous pemphigoid of childhood: autoantibodies target the same epitopes within the NC16A domain of BP180 as autoantibodies in bullous pemphigoid of adulthood.Arch Dermatol. 2000 Apr;136(4):527-32. doi: 10.1001/archderm.136.4.527. Arch Dermatol. 2000. PMID: 10768652 Review.
-
IgE-mediated mechanisms in bullous pemphigoid and other autoimmune bullous diseases.Expert Rev Clin Immunol. 2016;12(3):267-77. doi: 10.1586/1744666X.2016.1123092. Epub 2015 Dec 16. Expert Rev Clin Immunol. 2016. PMID: 26588556 Review.
Cited by
-
Single-cell transcriptomics analysis of bullous pemphigoid unveils immune-stromal crosstalk in type 2 inflammatory disease.Nat Commun. 2024 Jul 15;15(1):5949. doi: 10.1038/s41467-024-50283-3. Nat Commun. 2024. PMID: 39009587 Free PMC article.
-
Associated factors related to production of autoantibodies and dermo-epidermal separation in bullous pemphigoid.Arch Dermatol Res. 2025 Jan 24;317(1):303. doi: 10.1007/s00403-024-03760-0. Arch Dermatol Res. 2025. PMID: 39853516 Review.
-
Diagnostic utility of Th2 cytokines (IL-4, IL-5, IL-10, and IL-13) in pulpal blood for assessing pulpitis severity.BMC Oral Health. 2025 Apr 11;25(1):527. doi: 10.1186/s12903-025-05936-0. BMC Oral Health. 2025. PMID: 40217258 Free PMC article.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
