

Comparison of Pregnancy and Birth Outcomes Before vs During the COVID-19 Pandemic
- PMID: 35960517
- PMCID: PMC9375166
- DOI: 10.1001/jamanetworkopen.2022.26531
Comparison of Pregnancy and Birth Outcomes Before vs During the COVID-19 Pandemic
Erratum in
-
Errors in Abstract, Results, and Figure.JAMA Netw Open. 2022 Sep 1;5(9):e2233824. doi: 10.1001/jamanetworkopen.2022.33824. JAMA Netw Open. 2022. PMID: 36053541 Free PMC article. No abstract available.
-
Errors in Results, Discussion, Table 1, and the Supplement.JAMA Netw Open. 2023 May 1;6(5):e2314781. doi: 10.1001/jamanetworkopen.2023.14781. JAMA Netw Open. 2023. PMID: 37133866 Free PMC article. No abstract available.
Abstract
Importance: Little is known about changes in obstetric outcomes during the COVID-19 pandemic.
Objective: To assess whether obstetric outcomes and pregnancy-related complications changed during the COVID-19 pandemic.
Design, setting, and participants: This retrospective cohort study included pregnant patients receiving care at 463 US hospitals whose information appeared in the PINC AI Healthcare Database. The relative differences in birth outcomes, pregnancy-related complications, and length of stay (LOS) during the pandemic period (March 1, 2020, to April 31, 2021) were compared with the prepandemic period (January 1, 2019, to February 28, 2020) using logistic and Poisson models, adjusting for patients' characteristics, and comorbidities and with month and hospital fixed effects.
Exposures: COVID-19 pandemic period.
Main outcomes and measures: The 3 primary outcomes were the relative change in preterm vs term births, mortality outcomes, and mode of delivery. Secondary outcomes included the relative change in pregnancy-related complications and LOS.
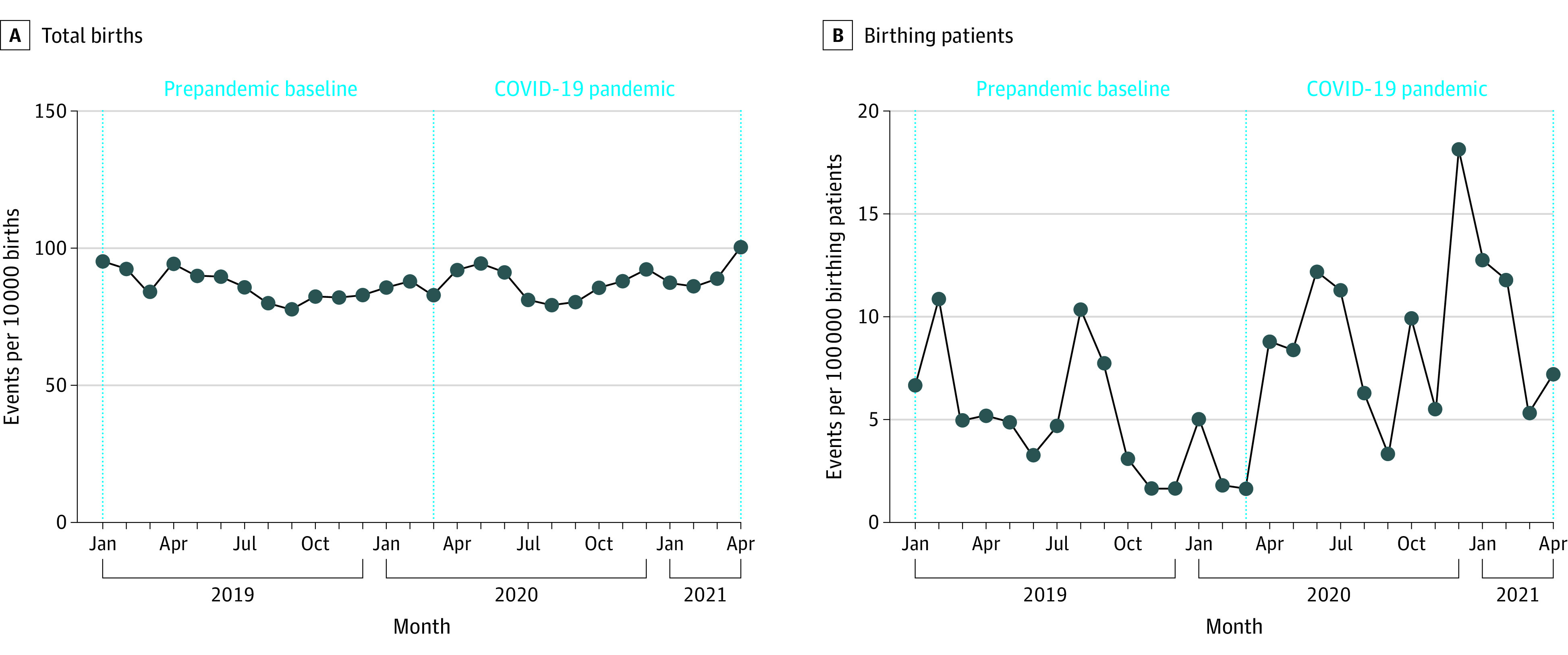
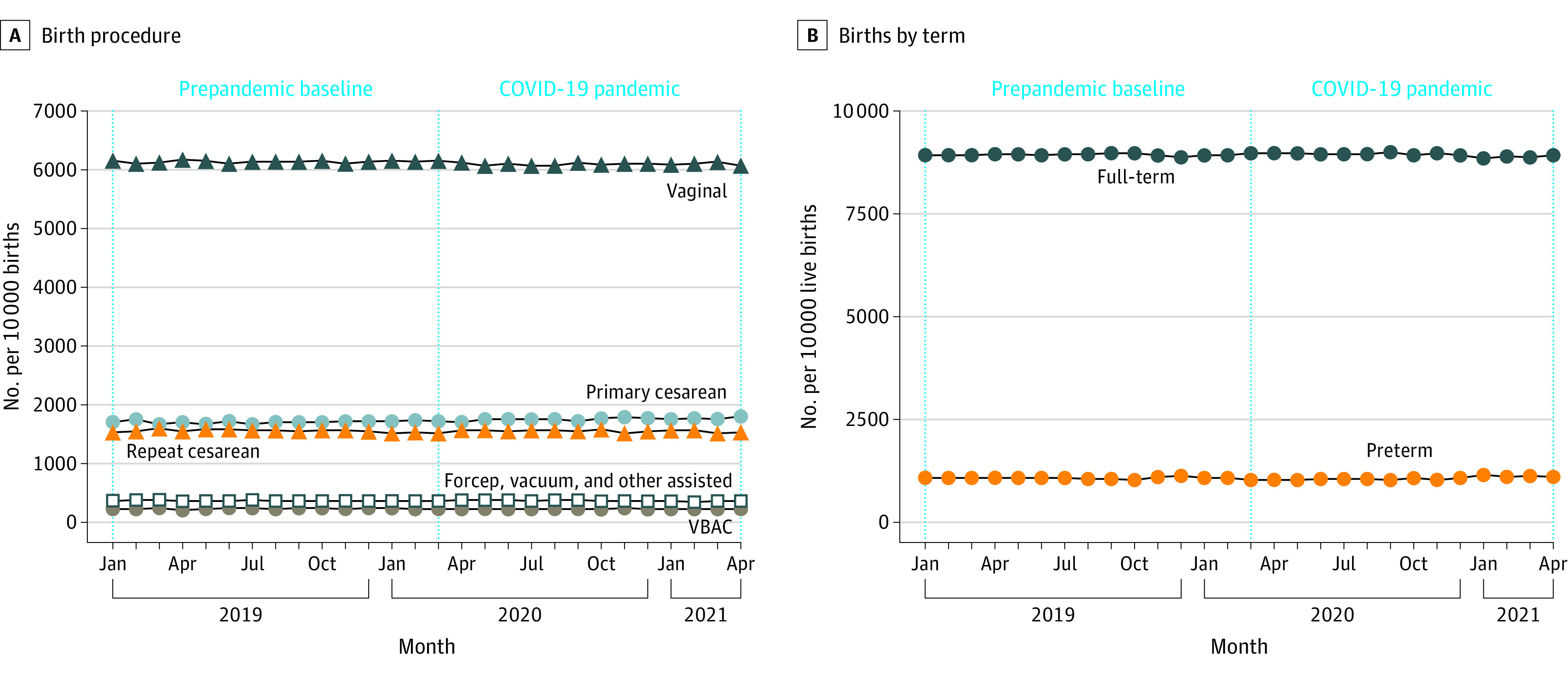
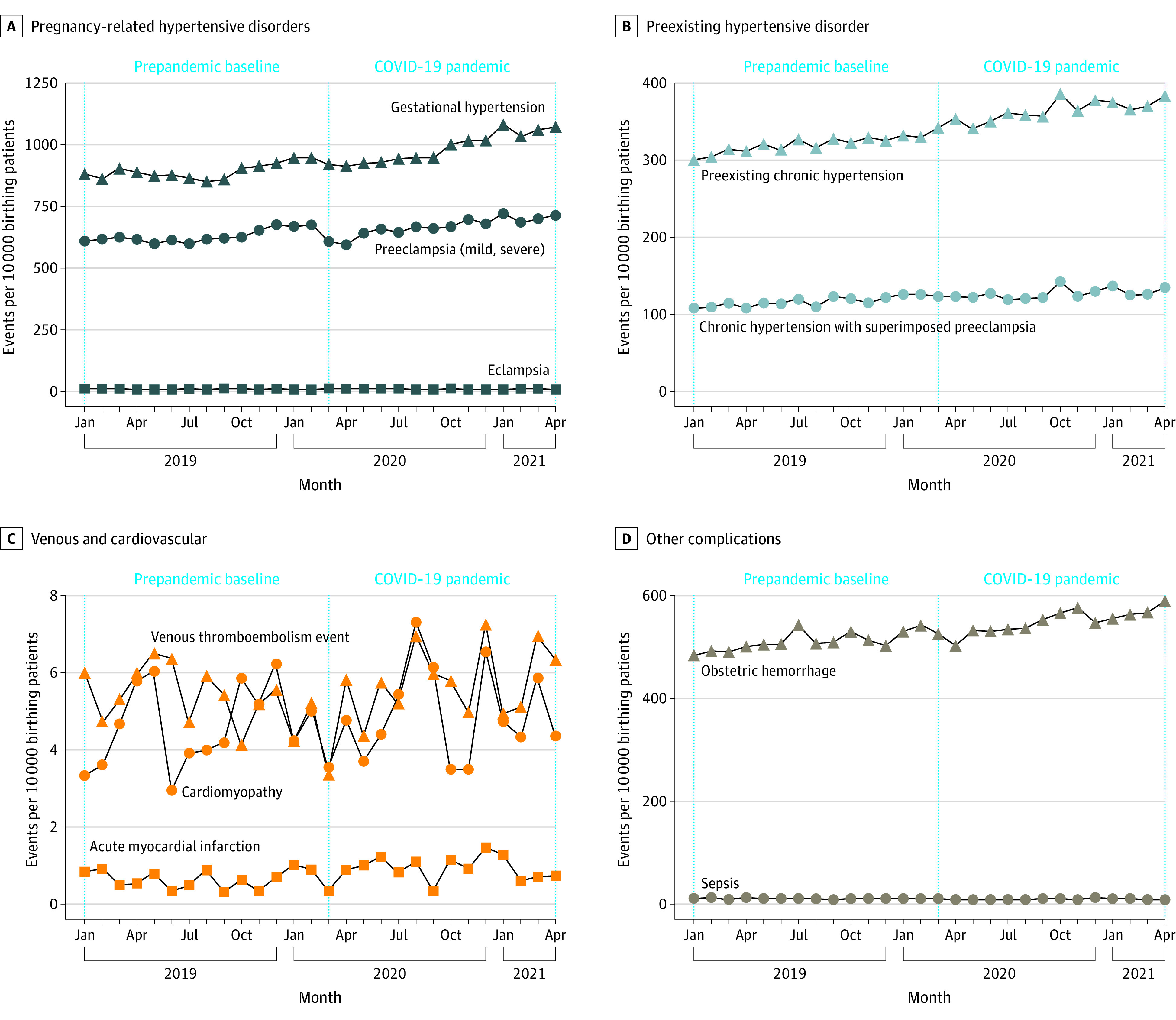
Results: There were 849 544 and 805 324 pregnant patients in the prepandemic and COVID-19 pandemic periods, respectively, and there were no significant differences in patient characteristics between periods, including age (≥35 years: 153 606 [18.1%] vs 148 274 [18.4%]), race and ethnicity (eg, Hispanic patients: 145 475 [47.1%] vs 143 905 [17.9%]; White patients: 456 014 [53.7%] vs 433 668 [53.9%]), insurance type (Medicaid: 366 233 [43.1%] vs 346 331 [43.0%]), and comorbidities (all standardized mean differences <0.10). There was a 5.2% decrease in live births during the pandemic. Maternal death during delivery hospitalization increased from 5.17 to 8.69 deaths per 100 000 pregnant patients (odds ratio [OR], 1.75; 95% CI, 1.19-2.58). There were minimal changes in mode of delivery (vaginal: OR, 1.01; 95% CI, 0.996-1.02; primary cesarean: OR, 1.02; 95% CI, 1.01-1.04; vaginal birth after cesarean: OR, 0.98; 95% CI, 0.95-1.00; repeated cesarean: OR, 0.96; 95% CI, 0.95-0.97). LOS during delivery hospitalization decreased by 7% (rate ratio, 0.931; 95% CI, 0.928-0.933). Lastly, the adjusted odds of gestational hypertension (OR, 1.08; 95% CI, 1.06-1.11), obstetric hemorrhage (OR, 1.07; 95% CI, 1.04-1.10), preeclampsia (OR, 1.04; 95% CI, 1.02-1.06), and preexisting chronic hypertension (OR, 1.06; 95% CI, 1.03-1.09) increased. No significant changes in preexisting racial and ethnic disparities were observed.
Conclusions and relevance: During the COVID-19 pandemic, there were increased odds of maternal death during delivery hospitalization, cardiovascular disorders, and obstetric hemorrhage. Further efforts are needed to ensure risks potentially associated with the COVID-19 pandemic do not persist beyond the current state of the pandemic.
Conflict of interest statement
Figures
References
-
- Aranda Z, Binde T, Tashman K, et al. ; Cross-site COVID-19 Syndromic Surveillance Working Group . Disruptions in maternal health service use during the COVID-19 pandemic in 2020: experiences from 37 health facilities in low-income and middle-income countries. BMJ Glob Health. 2022;7(1):e007247. doi:10.1136/bmjgh-2021-007247 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
