

Health Care Utilization in the 6 Months Following SARS-CoV-2 Infection
- PMID: 35960522
- PMCID: PMC9375168
- DOI: 10.1001/jamanetworkopen.2022.25657
Health Care Utilization in the 6 Months Following SARS-CoV-2 Infection
Abstract
Importance: After SARS-CoV-2 infection, many patients present with persistent symptoms for at least 6 months, collectively termed post-COVID conditions (PCC). However, the impact of PCC on health care utilization has not been well described.
Objectives: To estimate COVID-19-associated excess health care utilization following acute SARS-CoV-2 infection and describe utilization for select PCCs among patients who had positive SARS-CoV-2 test results (including reverse transcription-polymerase chain reaction and antigen tests) compared with control patients whose results were negative.
Design, setting, and participants: This matched retrospective cohort study included patients of all ages from 8 large integrated health care systems across the United States who completed a SARS-CoV-2 diagnostic test during March 1 to November 1, 2020. Patients were matched on age, sex, race and ethnicity, site, and date of SARS-CoV-2 test and were followed-up for 6 months. Data were analyzed from March 18, 2021, to June 8, 2022.
Exposure: SARS-CoV-2 infection.
Main outcomes and measures: Ratios of rate ratios (RRRs) for COVID-19-associated health care utilization were calculated with a difference-in-difference analysis using Poisson regression models. RRRs were estimated overall, by health care setting, by select population characteristics, and by 44 PCCs. COVID-19-associated excess health care utilization was estimated by health care setting.
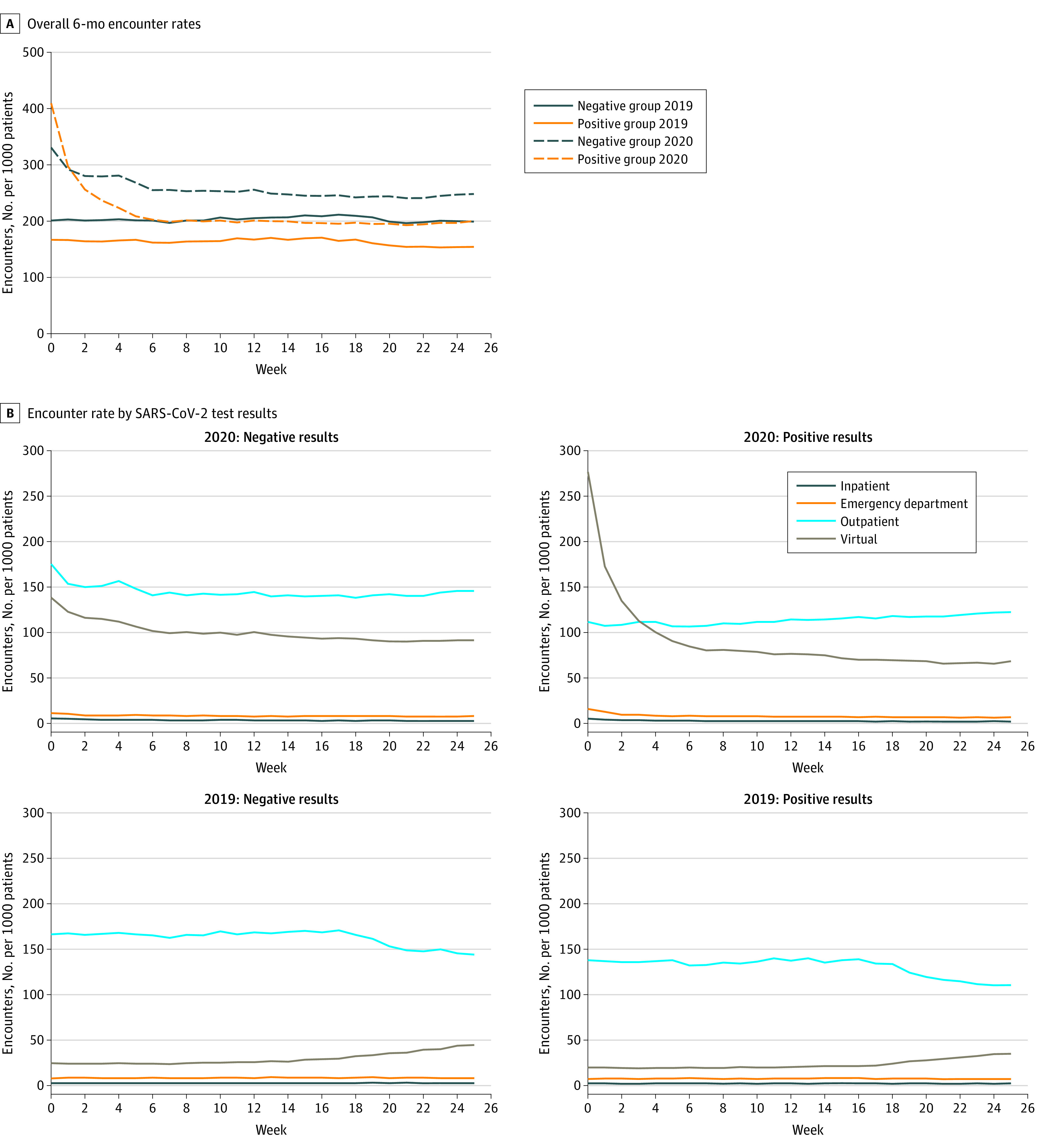
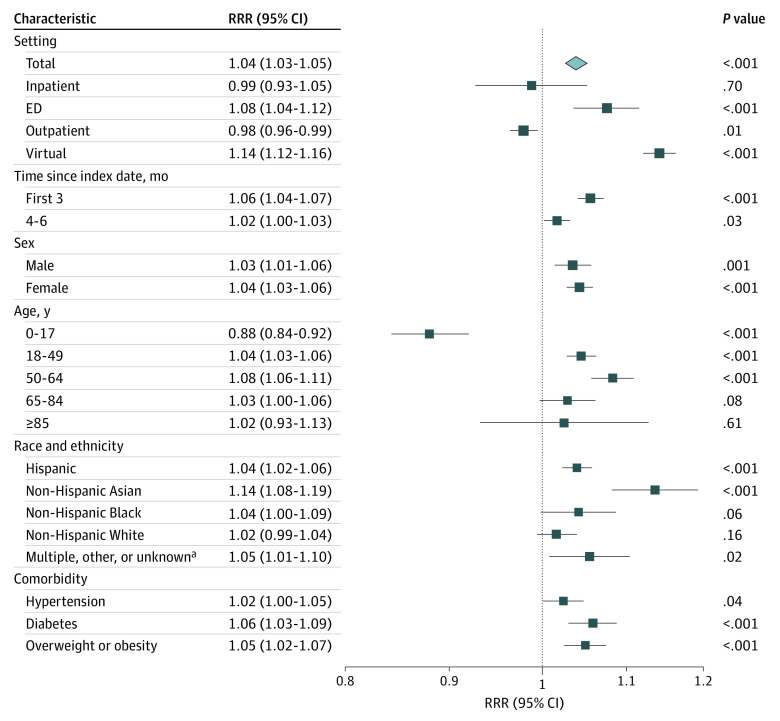
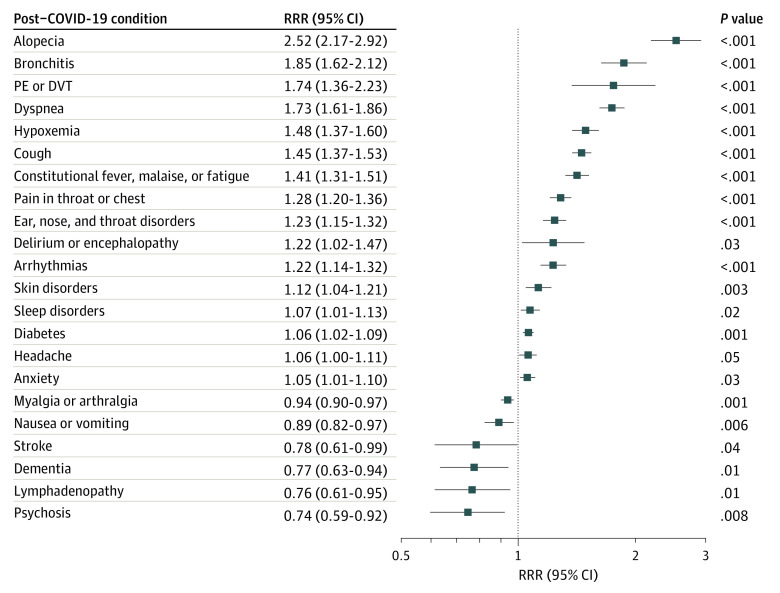
Results: The final matched cohort included 127 859 patients with test results positive for SARS-CoV-2 and 127 859 patients with test results negative for SARS-CoV-2. The mean (SD) age of the study population was 41.2 (18.6) years, 68 696 patients in each group (53.7%) were female, and each group included 66 211 Hispanic patients (51.8%), 9122 non-Hispanic Asian patients (7.1%), 7983 non-Hispanic Black patients (6.2%), and 34 326 non-Hispanic White patients (26.9%). Overall, SARS-CoV-2 infection was associated with a 4% increase in health care utilization over 6 months (RRR, 1.04 [95% CI, 1.03-1.05]), predominantly for virtual encounters (RRR, 1.14 [95% CI, 1.12-1.16]), followed by emergency department visits (RRR, 1.08 [95% CI, 1.04-1.12]). COVID-19-associated utilization for 18 PCCs remained elevated 6 months from the acute stage of infection, with the largest increase in COVID-19-associated utilization observed for infectious disease sequelae (RRR, 86.00 [95% CI, 5.07-1458.33]), COVID-19 (RRR, 19.47 [95% CI, 10.47-36.22]), alopecia (RRR, 2.52 [95% CI, 2.17-2.92]), bronchitis (RRR, 1.85 [95% CI, 1.62-2.12]), pulmonary embolism or deep vein thrombosis (RRR, 1.74 [95% CI, 1.36-2.23]), and dyspnea (RRR, 1.73 [95% CI, 1.61-1.86]). In total, COVID-19-associated excess health care utilization amounted to an estimated 27 217 additional medical encounters over 6 months (212.9 [95% CI, 146.5-278.4] visits per 1000 patients).
Conclusions and relevance: This cohort study documented an excess health care burden of PCC in the 6 months after the acute stage of infection. As health care systems evolve during a highly dynamic and ongoing global pandemic, these data provide valuable evidence to inform long-term strategic resource allocation for patients previously infected with SARS-CoV-2.
Conflict of interest statement
Figures
References
-
- Tenforde MW, Kim SS, Lindsell CJ, et al. ; IVY Network Investigators; CDC COVID-19 Response Team; IVY Network Investigators . Symptom duration and risk factors for delayed return to usual health among outpatients with COVID-19 in a multistate health care systems network—United States, March-June 2020. MMWR Morb Mortal Wkly Rep. 2020;69(30):993-998. doi:10.15585/mmwr.mm6930e1 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
