

Prognostic impact of NPM1 and FLT3 mutations in patients with AML in first remission treated with oral azacitidine
- PMID: 35960871
- PMCID: PMC10653004
- DOI: 10.1182/blood.2022016293
Prognostic impact of NPM1 and FLT3 mutations in patients with AML in first remission treated with oral azacitidine
Abstract
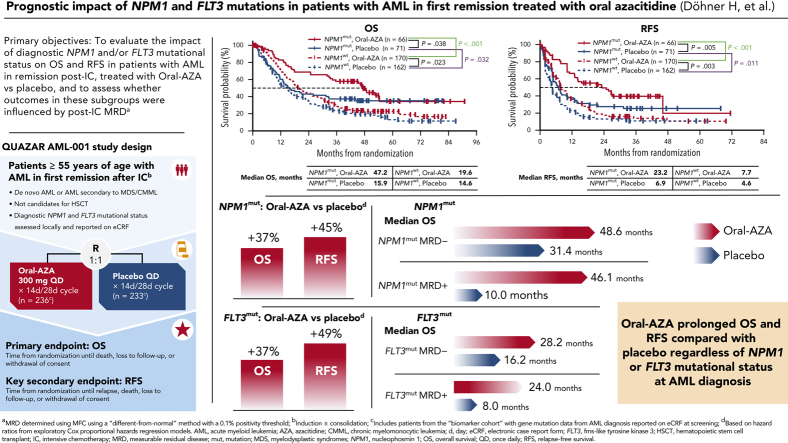
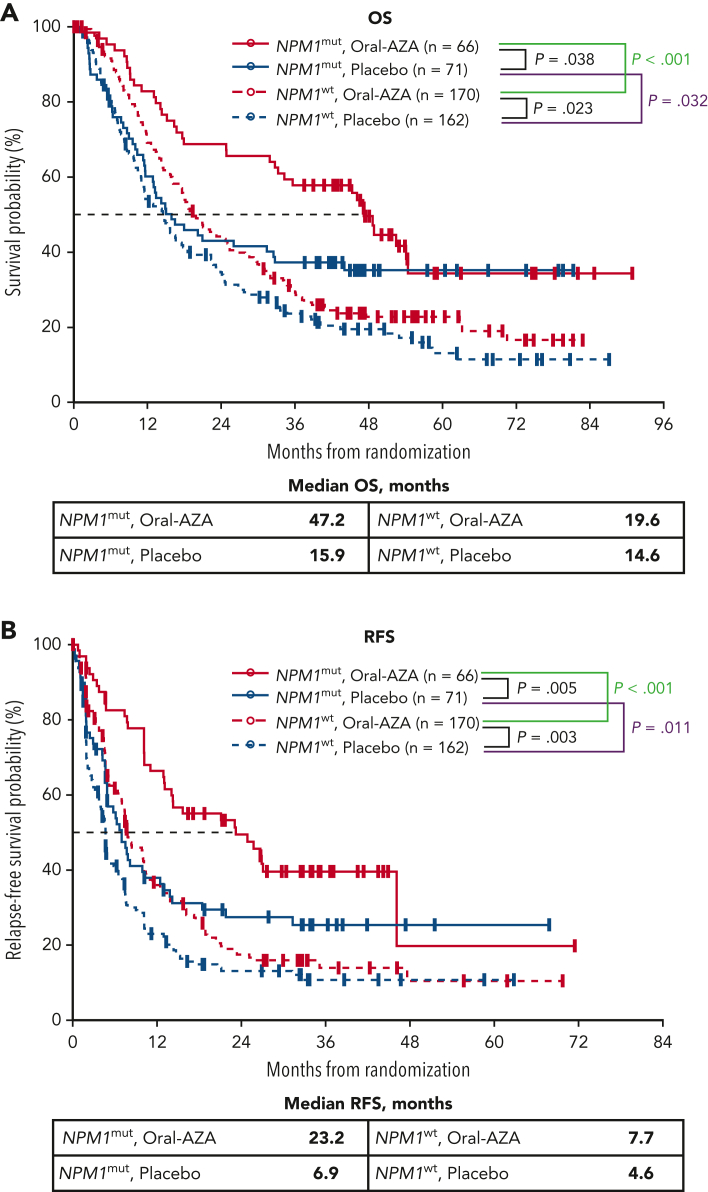
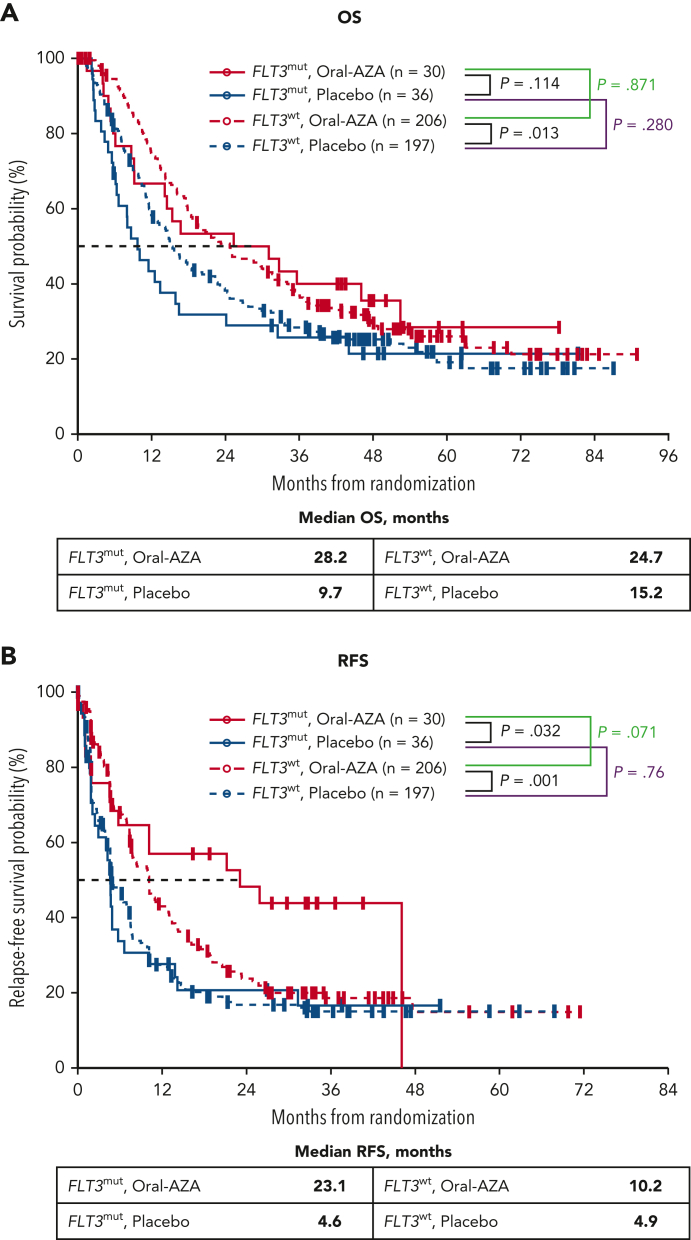
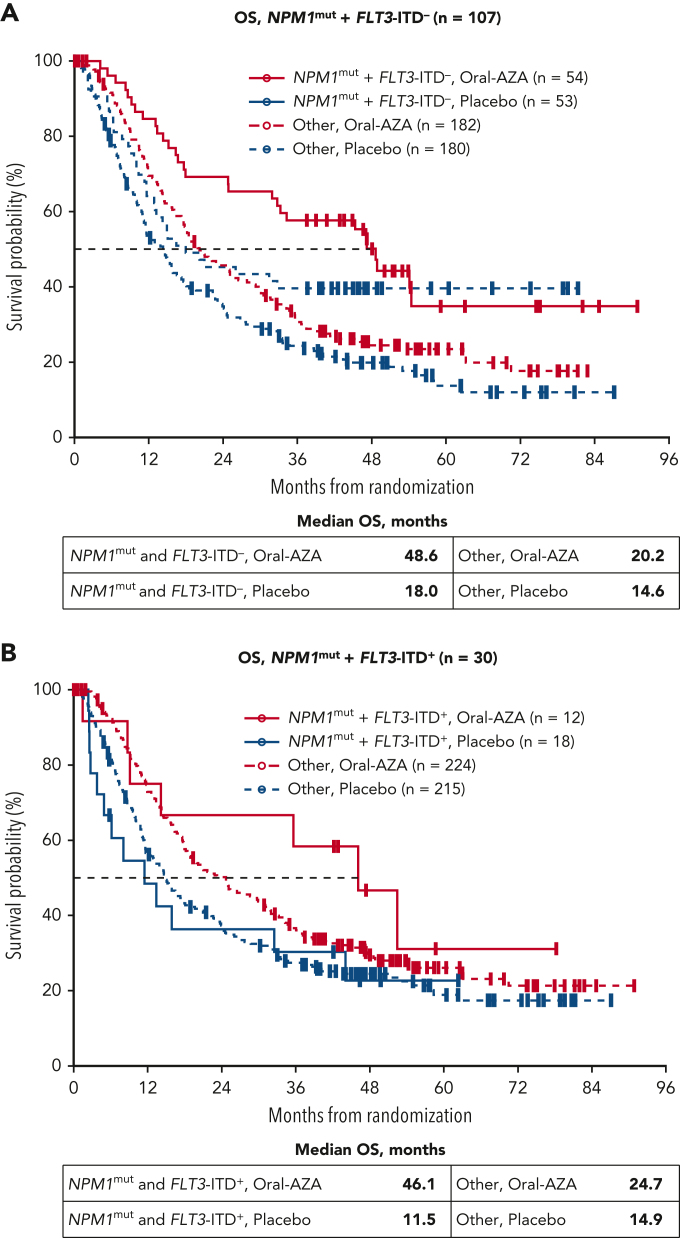
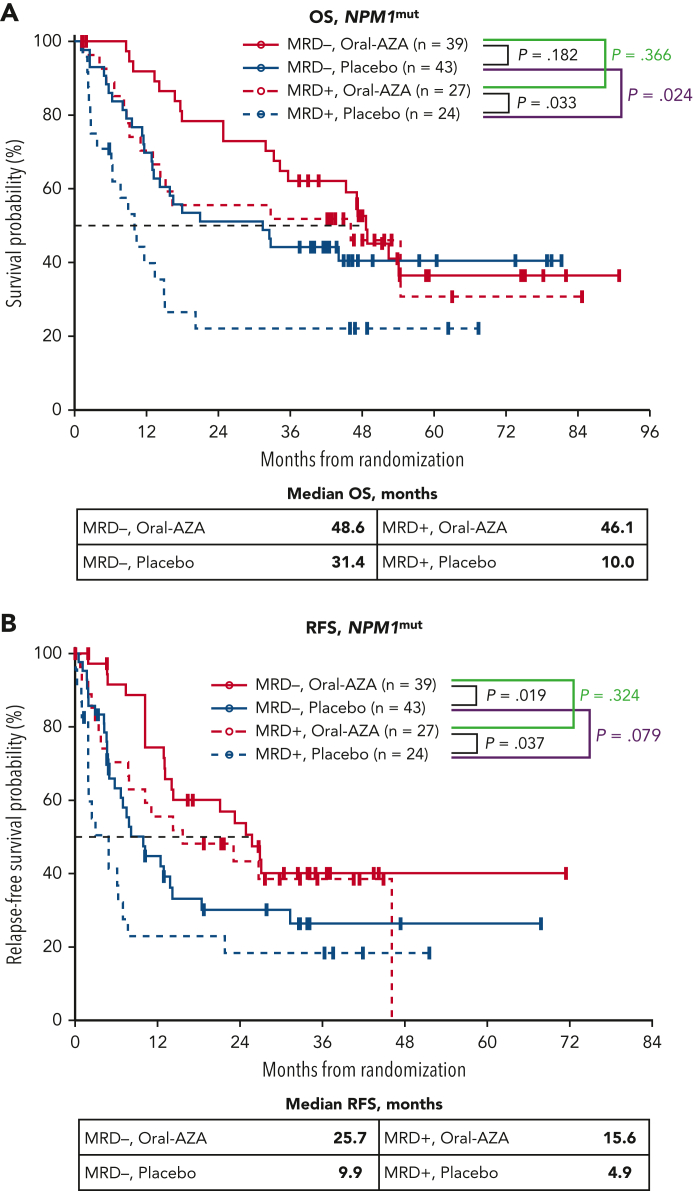
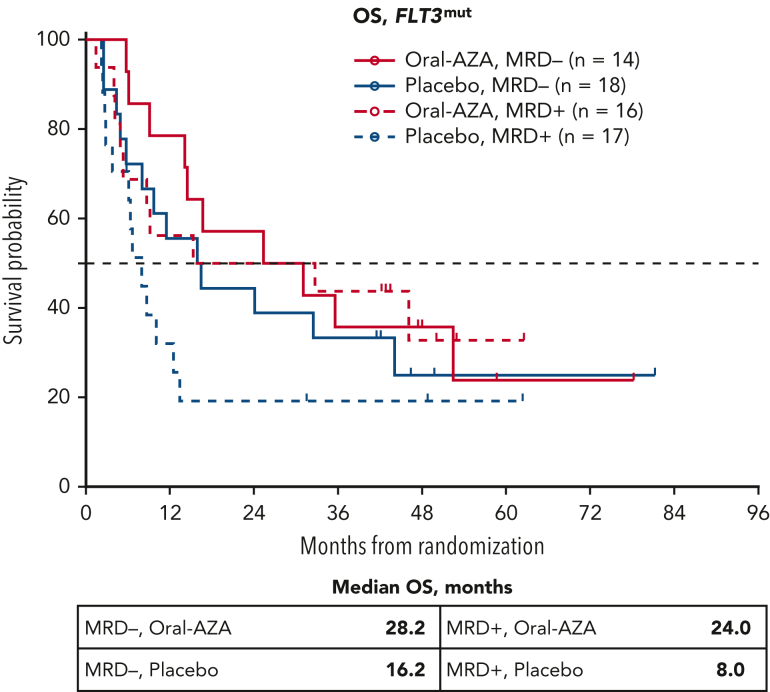
The randomized, placebo-controlled, phase 3 QUAZAR AML-001 trial (ClinicalTrials.gov identifier: NCT01757535) evaluated oral azacitidine (Oral-AZA) in patients with acute myeloid leukemia (AML) in first remission after intensive chemotherapy (IC) who were not candidates for hematopoietic stem cell transplantation. Eligible patients were randomized 1:1 to Oral-AZA 300 mg or placebo for 14 days per 28-day cycle. We evaluated relapse-free survival (RFS) and overall survival (OS) in patient subgroups defined by NPM1 and FLT3 mutational status at AML diagnosis and whether survival outcomes in these subgroups were influenced by presence of post-IC measurable residual disease (MRD). Gene mutations at diagnosis were collected from patient case report forms; MRD was determined centrally by multiparameter flow cytometry. Overall, 469 of 472 randomized patients (99.4%) had available mutational data; 137 patients (29.2%) had NPM1 mutations (NPM1mut), 66 patients (14.1%) had FLT3 mutations (FLT3mut; with internal tandem duplications [ITD], tyrosine kinase domain mutations [TKDmut], or both), and 30 patients (6.4%) had NPM1mut and FLT3-ITD at diagnosis. Among patients with NPM1mut, OS and RFS were improved with Oral-AZA by 37% (hazard ratio [HR], 0.63; 95% confidence interval [CI], 0.41-0.98) and 45% (HR, 0.55; 95% CI, 0.35-0.84), respectively, vs placebo. Median OS was improved numerically with Oral-AZA among patients with NPM1mut whether without MRD (48.6 months vs 31.4 months with placebo) or with MRD (46.1 months vs 10.0 months with placebo) post-IC. Among patients with FLT3mut, Oral-AZA improved OS and RFS by 37% (HR, 0.63; 95% CI, 0.35-1.12) and 49% (HR, 0.51; 95% CI, 0.27-0.95), respectively, vs placebo. Median OS with Oral-AZA vs placebo was 28.2 months vs 16.2 months, respectively, for patients with FLT3mut and without MRD and 24.0 months vs 8.0 months for patients with FLT3mut and MRD. In multivariate analyses, Oral-AZA significantly improved survival independent of NPM1 or FLT3 mutational status, cytogenetic risk, or post-IC MRD status.
© 2022 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: H. Döhner received honoraria from and served as a consultant to AbbVie, Agios, Amgen, Astellas, AstraZeneca, Berlin-Chemie, BMS, Celgene, GEMoaB, Gilead, Janssen, Jazz, Novartis, and Syndax; received research funding from AbbVie, Agios, Amgen, Astellas, BMS, Celgene, Jazz Pharmaceuticals, Kronos Bio, and Novartis; and received travel expenses from Servier. A.H.W. served on the speaker’s bureau and advisory board of and received travel expenses from BMS. G.J.R. served as a consultant to or on the advisory board or data and safety monitoring committee of AbbVie, Agios, Amgen, Astellas, AstraZeneca, BMS, Blueprint Medicines, bluebird bio, Celgene, GSK, Janssen, Jasper Therapeutics, Jazz, MEI Pharma (IDMC Chair), Mesoblast, Novartis, Pfizer, Syndax, and Takeda (IRC Chair); and received research support from Janssen. P.M. served as a consultant to, received research funding from, and served on the speaker’s bureau of BMS. F.R.T. served on the advisory board of AbbVie, Astellas, BMS/Celgene, Jazz, Novartis, and Pfizer; and received research support from BMS/Celgene and Novartis. F.R. received research funding from and served on the advisory board of BMS/Celgene. H. Dombret received honoraria from Incyte. K.P. received research funding from BMS/Celgene, Incyte, and Novartis. I.S. served as a consultant to and on the advisory board of Amgen, BMS/Celgene, Janssen, Kite/Gilead, Pfizer, Sanofi, and Takeda; and has stock ownership in illumiSonics Inc. B.S. is employed by BMS. W.L.S. is a contractor for and has a patent filed with BMS. M.U. is employed by and has a patent filed with BMS. A.R., A.T., and D.L.d.M. are employed by, have stock ownership in, and have a patent filed with BMS. E.T.C. and C.L.B. are employed by and have stock ownership in BMS.
Figures
Comment in
-
By any other name ….Blood. 2022 Oct 13;140(15):1657-1658. doi: 10.1182/blood.2022018005. Blood. 2022. PMID: 36227747 No abstract available.
References
-
- Yang JJ, Park TS, Wan TS. Recurrent cytogenetic abnormalities in acute myeloid leukemia. Methods Mol Biol. 2017;1541:223–245. - PubMed
-
- Döhner H, Weisdorf DJ, Bloomfield CD. Acute myeloid leukemia. N Engl J Med. 2015;373(12):1136–1152. - PubMed
-
- Estey EH. Acute myeloid leukemia: 2021 update on risk-stratification and management. Am J Hematol. 2020;95(11):1368–1398. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
