

Carbon Dioxide, Blood Pressure, and Perioperative Stroke: A Retrospective Case-Control Study
- PMID: 35960872
- PMCID: PMC10324342
- DOI: 10.1097/ALN.0000000000004354
Carbon Dioxide, Blood Pressure, and Perioperative Stroke: A Retrospective Case-Control Study
Abstract
Background: The relationship between intraoperative physiology and postoperative stroke is incompletely understood. Preliminary data suggest that either hypo- or hypercapnia coupled with reduced cerebrovascular inflow (e.g., due to hypotension) can lead to ischemia. This study tested the hypothesis that the combination of intraoperative hypotension and either hypo- or hypercarbia is associated with postoperative ischemic stroke.
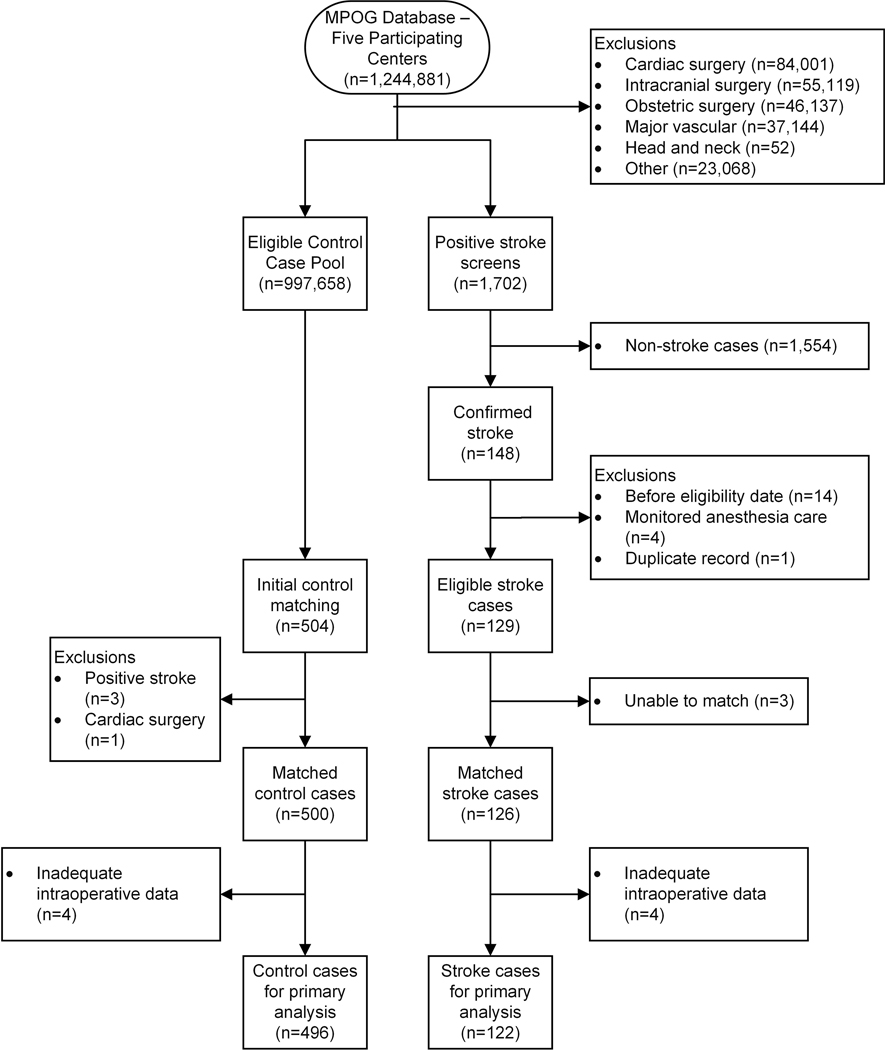
Methods: We conducted a retrospective, case-control study via the Multicenter Perioperative Outcomes Group. Noncardiac, nonintracranial, and nonmajor vascular surgical cases (18 yr or older) were extracted from five major academic centers between January 2004 and December 2015. Ischemic stroke cases were identified via manual chart review and matched to controls (1:4). Time and reduction below key mean arterial blood pressure thresholds (less than 55 mmHg, less than 60 mmHg, less than 65 mmHg) and outside of specific end-tidal carbon dioxide thresholds (30 mmHg or less, 35 mmHg or less, 45 mmHg or greater) were calculated based on total area under the curve. The association between stroke and total area under the curve values was then tested while adjusting for relevant confounders.
Results: In total, 1,244,881 cases were analyzed. Among the cases that screened positive for stroke (n = 1,702), 126 were confirmed and successfully matched with 500 corresponding controls. Total area under the curve was significantly associated with stroke for all thresholds tested, with the strongest combination observed with mean arterial pressure less than 55 mmHg (adjusted odds ratio per 10 mmHg-min, 1.17 [95% CI, 1.10 to 1.23], P < 0.0001) and end-tidal carbon dioxide 45 mmHg or greater (adjusted odds ratio per 10 mmHg-min, 1.11 [95% CI, 1.10 to 1.11], P < 0.0001). There was no interaction effect observed between blood pressure and carbon dioxide.
Conclusions: Intraoperative hypotension and carbon dioxide dysregulation may each independently increase postoperative stroke risk.
Copyright © 2022, the American Society of Anesthesiologists. All Rights Reserved.
Conflict of interest statement
Dr. Colquhoun has research funding (unrelated to presented work) from Merck & Co., Inc., paid to the University of Michigan. Dr. Mashour is a consultant for TRYP Therapeutics, San Diego, CA, and Dr. Vlisides receives support from Blue Cross Blue Shield of Michigan for research unrelated to this work.
Figures
Comment in
-
Carbon Dioxide, Blood Pressure, and Stroke: Comment.Anesthesiology. 2023 Aug 1;139(2):228-229. doi: 10.1097/ALN.0000000000004544. Anesthesiology. 2023. PMID: 37011017 No abstract available.
References
-
- Mashour GA, Shanks AM, Kheterpal S: Perioperative stroke and associated mortality after noncardiac, nonneurologic surgery. Anesthesiology 2011; 114: 1289–96 - PubMed
-
- Perioperative covert stroke in patients undergoing non-cardiac surgery (NeuroVISION): A prospective cohort study. Lancet 2019; 394: 1022–29 - PubMed
-
- Saltman AP, Silver FL, Fang J, Stamplecoski M, Kapral MK: Care and outcomes of patients with in-hospital stroke. JAMA Neurol 2015; 72: 749–55 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
