

Prognostic validation of a new classification system for extent of resection in glioblastoma: A report of the RANO resect group
- PMID: 35961053
- PMCID: PMC10158281
- DOI: 10.1093/neuonc/noac193
Prognostic validation of a new classification system for extent of resection in glioblastoma: A report of the RANO resect group
Abstract
Background: Terminology to describe extent of resection in glioblastoma is inconsistent across clinical trials. A surgical classification system was previously proposed based upon residual contrast-enhancing (CE) tumor. We aimed to (1) explore the prognostic utility of the classification system and (2) define how much removed non-CE tumor translates into a survival benefit.
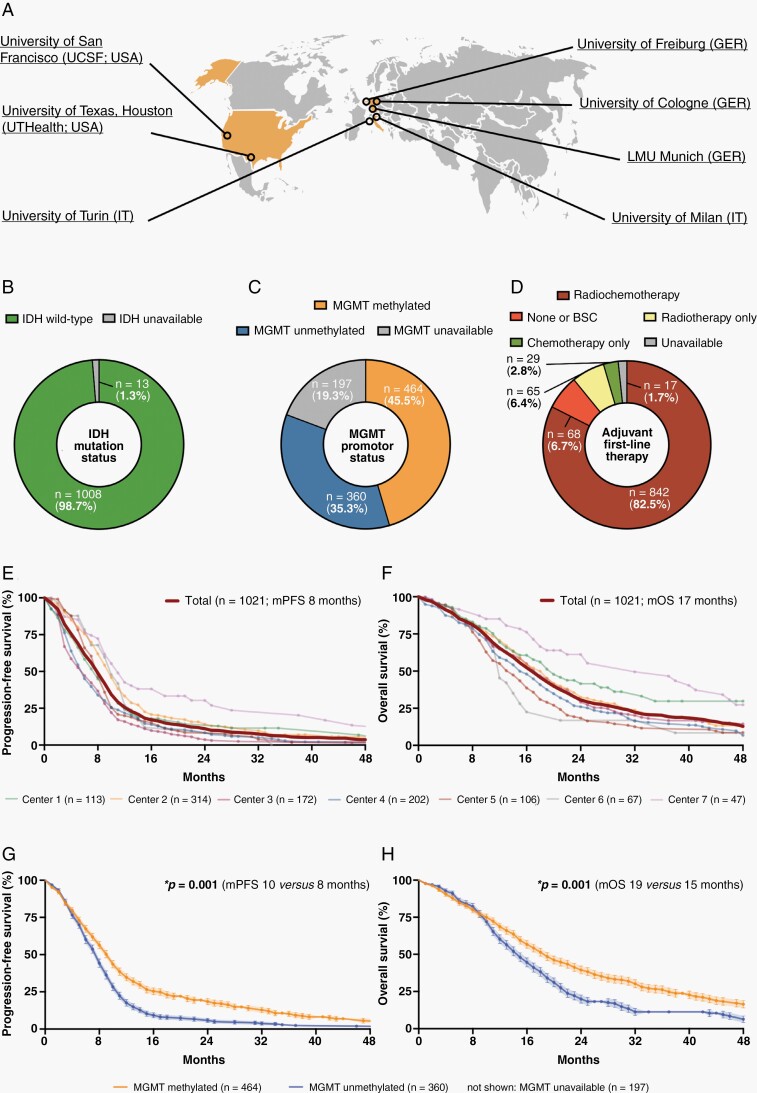
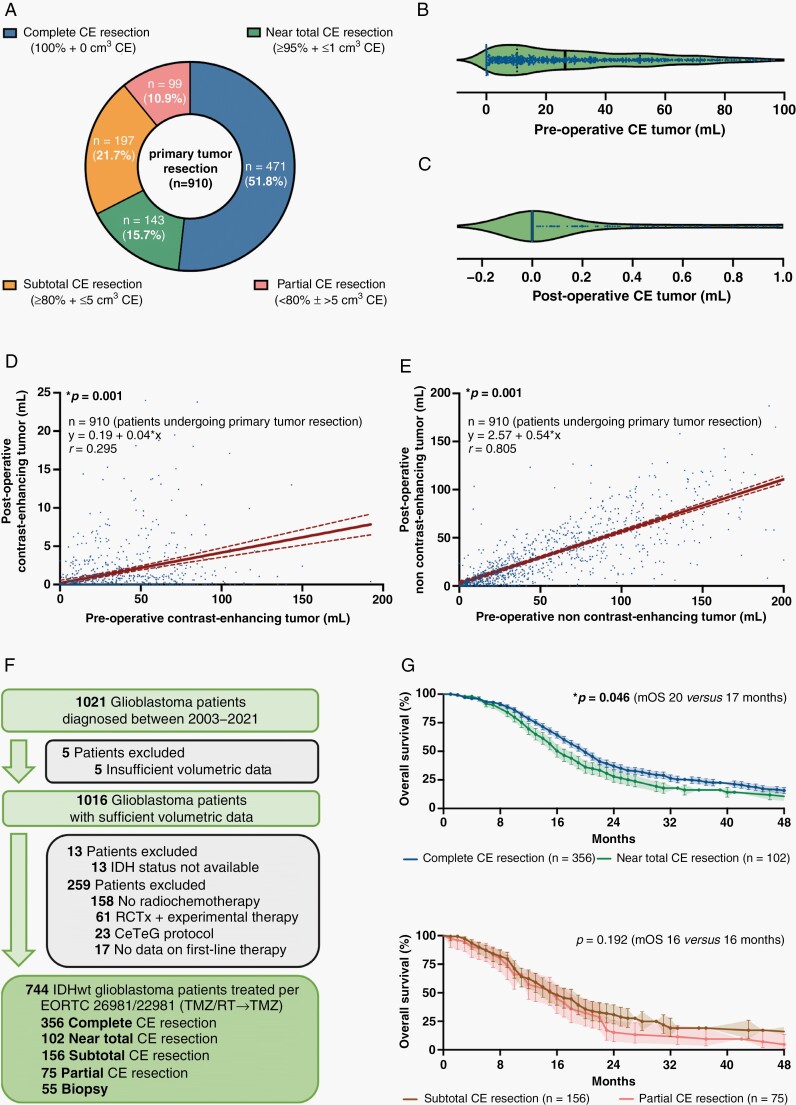
Methods: The international RANO resect group retrospectively searched previously compiled databases from 7 neuro-oncological centers in the USA and Europe for patients with newly diagnosed glioblastoma per WHO 2021 classification. Clinical and volumetric information from pre- and postoperative MRI were collected.
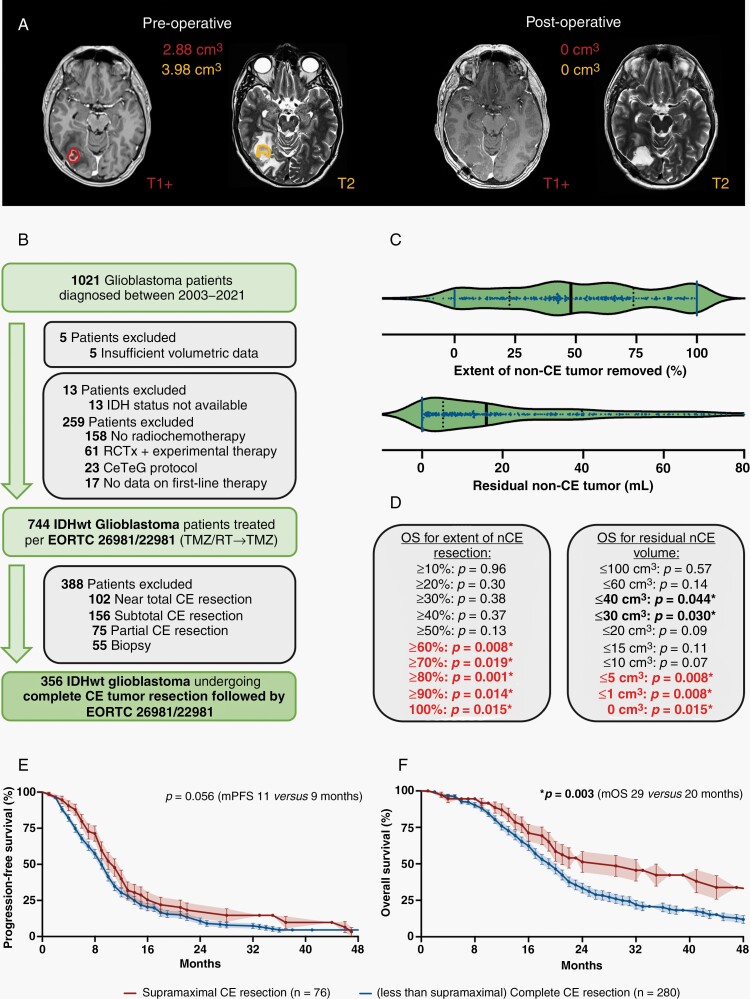
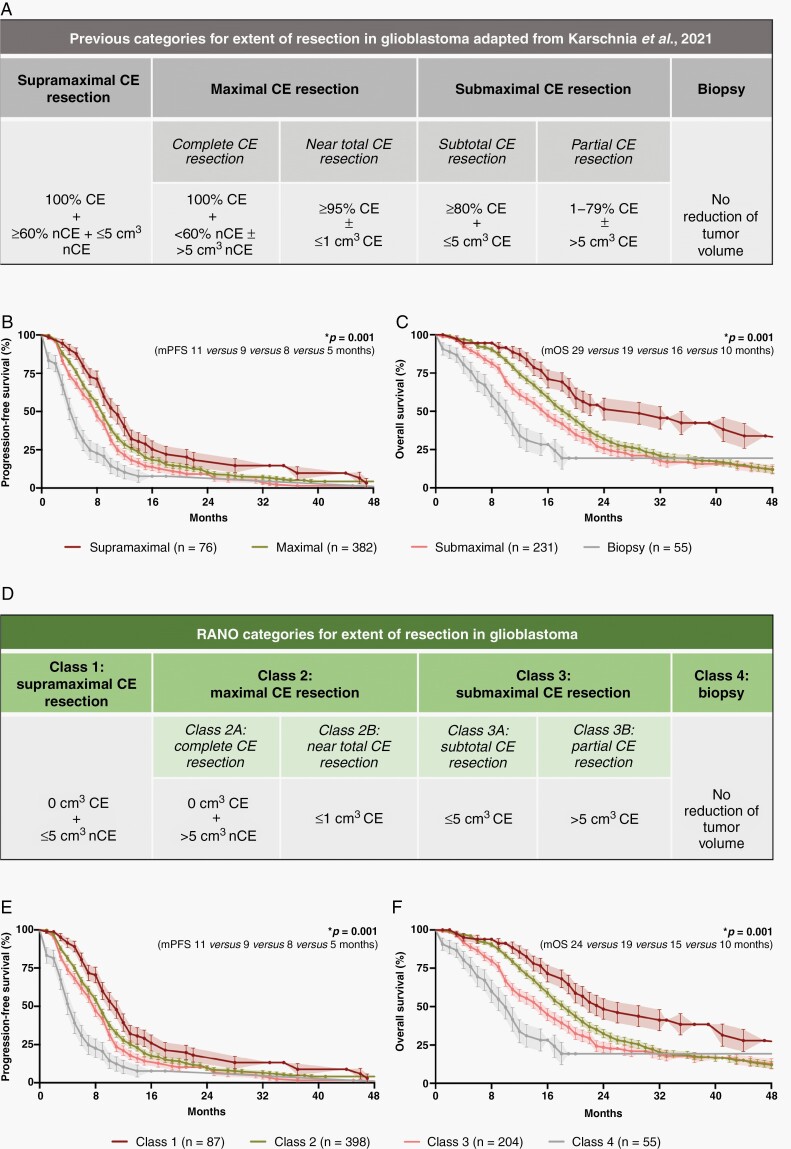
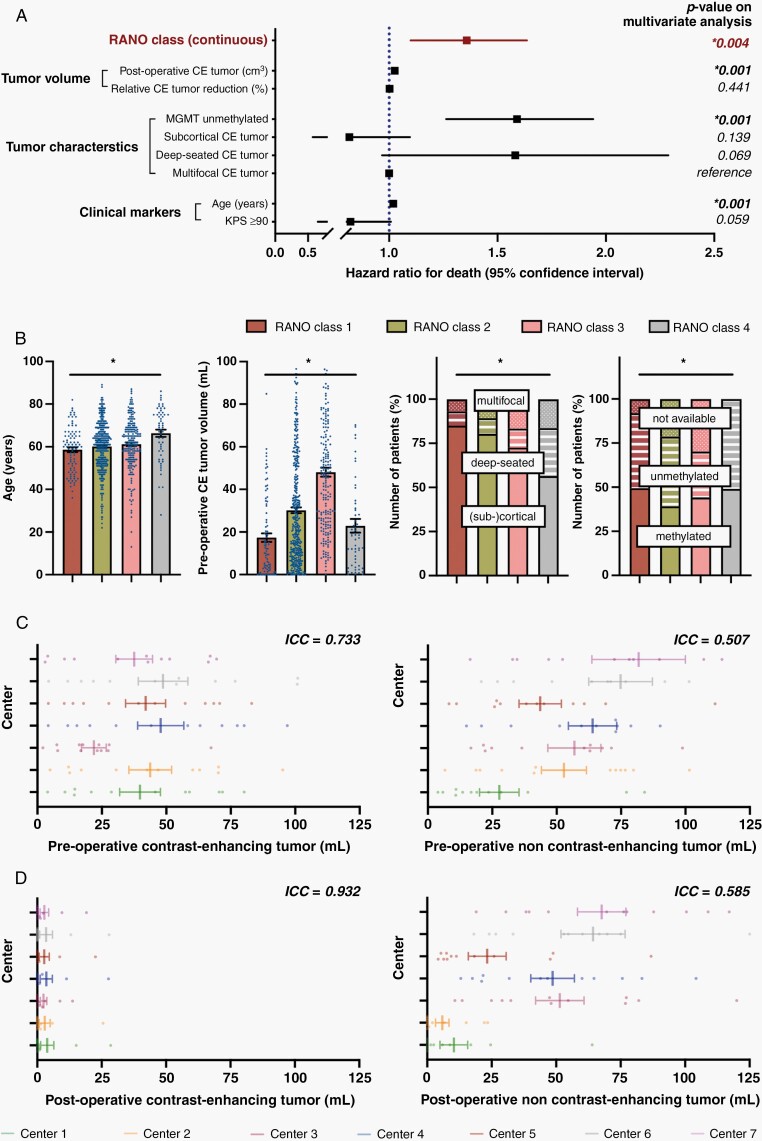
Results: We collected 1,008 patients with newly diagnosed IDHwt glioblastoma. 744 IDHwt glioblastomas were treated with radiochemotherapy per EORTC-26981/22981 (TMZ/RT→TMZ) following surgery. Among these homogenously treated patients, lower absolute residual tumor volumes (in cm3) were favorably associated with outcome: patients with "maximal CE resection" (class 2) had superior outcome compared to patients with "submaximal CE resection" (class 3) or "biopsy" (class 4). Extensive resection of non-CE tumor (≤5 cm3 residual non-CE tumor) was associated with better survival among patients with complete CE resection, thus defining class 1 ("supramaximal CE resection"). The prognostic value of the resection classes was retained on multivariate analysis when adjusting for molecular and clinical markers.
Conclusions: The proposed "RANO categories for extent of resection in glioblastoma" are highly prognostic and may serve for stratification within clinical trials. Removal of non-CE tumor beyond the CE tumor borders may translate into additional survival benefit, providing a rationale to explicitly denominate such "supramaximal CE resection."
Keywords: EOR; classification; glioblastoma; outcome; surgical resection.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Society for Neuro-Oncology.
Figures
Comment in
-
Rethinking classification and categorization of resection extent and its impact on patient survival in glioblastoma: Was Walter Dandy ahead of his time?Neuro Oncol. 2023 May 4;25(5):955-957. doi: 10.1093/neuonc/noad013. Neuro Oncol. 2023. PMID: 36645373 Free PMC article. No abstract available.
