

Infant BCG vaccination and risk of pulmonary and extrapulmonary tuberculosis throughout the life course: a systematic review and individual participant data meta-analysis
- PMID: 35961354
- PMCID: PMC10406427
- DOI: 10.1016/S2214-109X(22)00283-2
Infant BCG vaccination and risk of pulmonary and extrapulmonary tuberculosis throughout the life course: a systematic review and individual participant data meta-analysis
Abstract
Background: BCG vaccines are given to more than 100 million children every year, but there is considerable debate regarding the effectiveness of BCG vaccination in preventing tuberculosis and death, particularly among older children and adults. We therefore aimed to investigate the age-specific impact of infant BCG vaccination on tuberculosis (pulmonary and extrapulmonary) development and mortality.
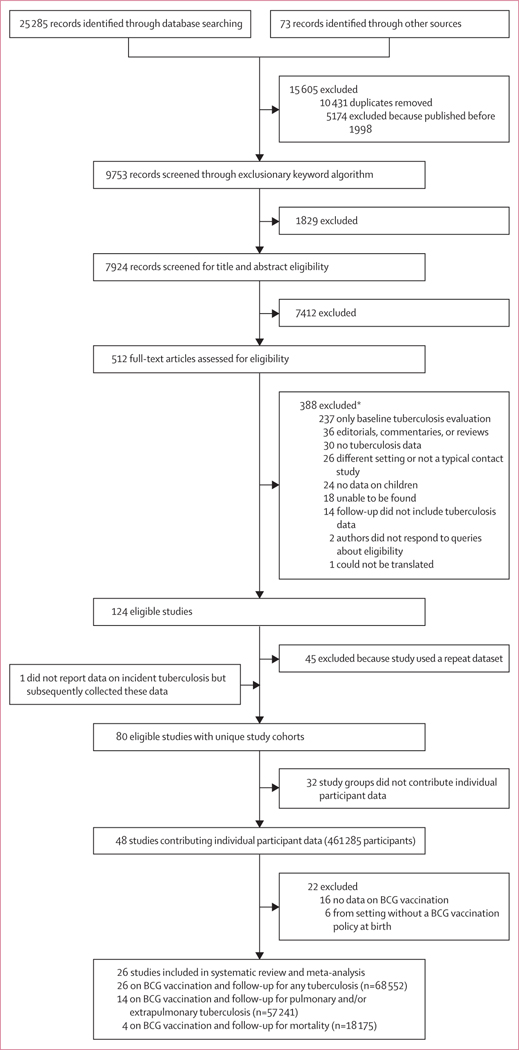
Methods: In this systematic review and individual participant data meta-analysis, we searched MEDLINE, Web of Science, BIOSIS, and Embase without language restrictions for case-contact cohort studies of tuberculosis contacts published between Jan 1, 1998, and April 7, 2018. Search terms included "mycobacterium tuberculosis", "TB", "tuberculosis", and "contact". We excluded cohort studies that did not provide information on BCG vaccination or were done in countries that did not recommend BCG vaccination at birth. Individual-level participant data for a prespecified list of variables, including the characteristics of the exposed participant (contact), the index case, and the environment, were requested from authors of all eligible studies. Our primary outcome was a composite of prevalent (diagnosed at or within 90 days of baseline) and incident (diagnosed more than 90 days after baseline) tuberculosis in contacts exposed to tuberculosis. Secondary outcomes were pulmonary tuberculosis, extrapulmonary tuberculosis, and mortality. We derived adjusted odds ratios (aORs) using mixed-effects, binary, multivariable logistic regression analyses with study-level random effects, adjusting for the variable of interest, baseline age, sex, previous tuberculosis, and whether data were collected prospectively or retrospectively. We stratified our results by contact age and Mycobacterium tuberculosis infection status. This study is registered with PROSPERO, CRD42020180512.
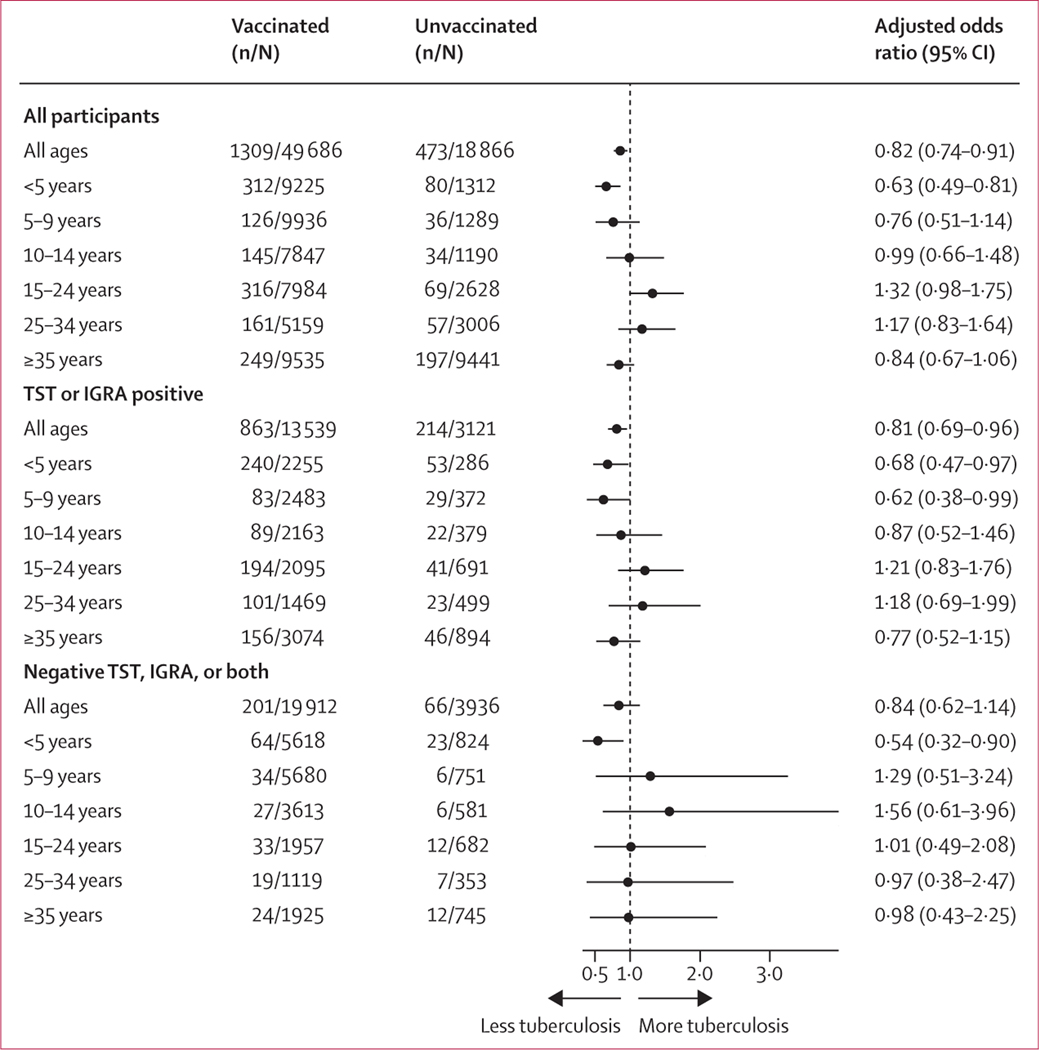
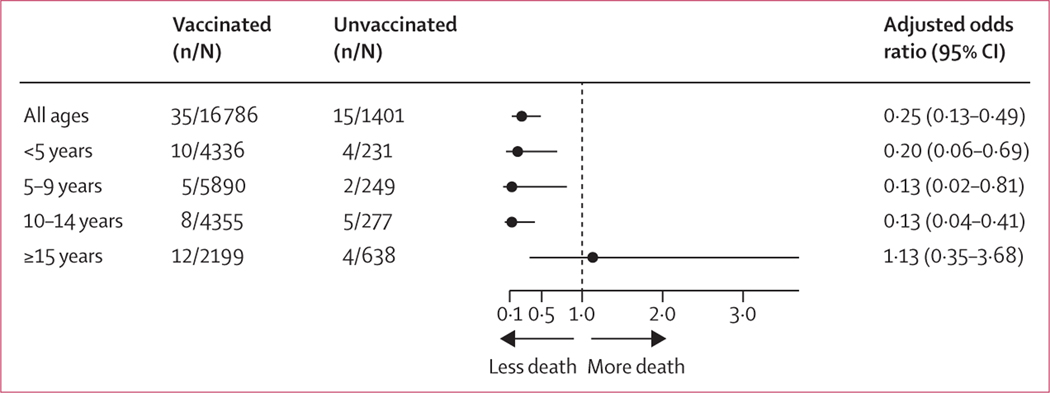
Findings: We identified 14 927 original records from our database searches. We included participant-level data from 26 cohort studies done in 17 countries in our meta-analysis. Among 68 552 participants, 1782 (2·6%) developed tuberculosis (1309 [2·6%] of 49 686 BCG-vaccinated participants vs 473 [2·5%] of 18 866 unvaccinated participants). The overall effectiveness of BCG vaccination against all tuberculosis was 18% (aOR 0·82, 95% CI 0·74-0·91). When stratified by age, BCG vaccination only significantly protected against all tuberculosis in children younger than 5 years (aOR 0·63, 95% CI 0·49-0·81). Among contacts with a positive tuberculin skin test or IFNγ release assay, BCG vaccination significantly protected against tuberculosis among all participants (aOR 0·81, 95% CI 0·69-0·96), participants younger than 5 years (0·68, 0·47-0·97), and participants aged 5-9 years (0·62, 0·38-0·99). There was no protective effect among those with negative tests, unless they were younger than 5 years (0·54, 0·32-0·90). 14 cohorts reported on whether tuberculosis was pulmonary or extrapulmonary (n=57 421). BCG vaccination significantly protected against pulmonary tuberculosis among all participants (916 [2·2%] in 41 119 vaccinated participants vs 334 [2·1%] in 16 161 unvaccinated participants; aOR 0·81, 0·70-0·94) but not against extrapulmonary tuberculosis (106 [0·3%] in 40 318 vaccinated participants vs 38 [0·2%] in 15 865 unvaccinated participants; 0·96, 0·65-1·41). In the four studies with mortality data, BCG vaccination was significantly protective against death (0·25, 0·13-0·49).
Interpretation: Our results suggest that BCG vaccination at birth is effective at preventing tuberculosis in young children but is ineffective in adolescents and adults. Immunoprotection therefore needs to be boosted in older populations.
Funding: National Institutes of Health.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
Comment in
-
Infant BCG vaccination is beneficial, but not sufficient.Lancet Glob Health. 2022 Sep;10(9):e1220-e1221. doi: 10.1016/S2214-109X(22)00325-4. Lancet Glob Health. 2022. PMID: 35961334 No abstract available.
References
-
- WHO. Weekly epidemiological record. July 14, 2017. https://apps.who.int/iris/bitstream/handle/10665/255870/WER9228.pdf (accessed May 1, 2021).
-
- Rieder HL. BCG vaccination. In: Davies P, Barnes P, Gordon S, eds. Clinical tuberculosis, 4th edn. London: Hodder Arnold, 2008: 411–27.
-
- Trunz BB, Fine P, Dye C. Effect of BCG vaccination on childhood tuberculous meningitis and miliary tuberculosis worldwide: a meta-analysis and assessment of cost-effectiveness. Lancet 2006; 367: 1173–80. - PubMed
-
- Fine PE. BCG: the challenge continues. Scand J Infect Dis 2001; 33: 243–45. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
