

Splenic artery embolization changes the management of blunt splenic injury: an observational analysis of 680 patients graded by the revised 2018 AAST-OIS
- PMID: 35962229
- PMCID: PMC9839812
- DOI: 10.1007/s00464-022-09531-0
Splenic artery embolization changes the management of blunt splenic injury: an observational analysis of 680 patients graded by the revised 2018 AAST-OIS
Abstract
Background: This study aimed to evaluate the management of blunt splenic injury (BSI) and highlight the role of splenic artery embolization (SAE).
Methods: We conducted a retrospective review of all patients with BSI over 15 years. Splenic injuries were graded by the 2018 revision of the American Association for the Surgery of Trauma-Organ Injury Scale (AAST-OIS). Our hospital provide 24/7 in-house surgeries and 24/7 in-house interventional radiology facility. Patients with BSI who arrived hypotensive and were refractory to resuscitation required surgery and patients with vascular injury on abdominal computed tomography were considered for SAE.
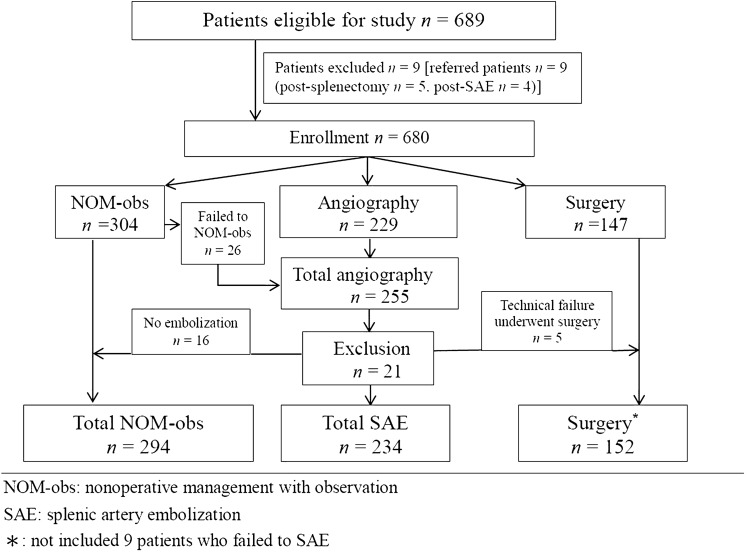
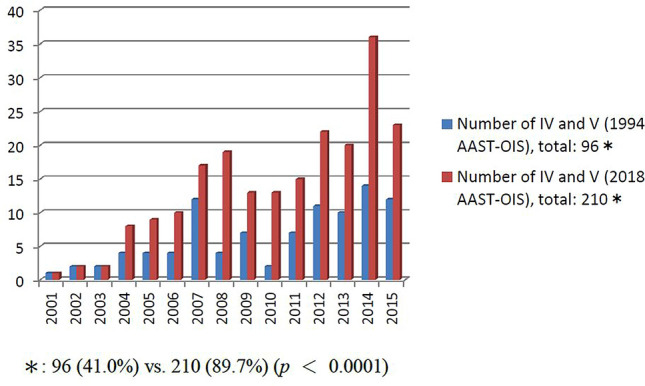
Results: In total, 680 patients with BSI, the number of patients who underwent nonoperative management with observation (NOM-obs), SAE, and surgery was 294, 234, and 152, respectively. The number of SAEs increased from 4 (8.3%) in 2001 to 23 (60.5%) in 2015 (p < 0.0001); conversely, the number of surgeries decreased from 21 (43.8%) in 2001 to 4 (10.5%) in 2015 (p = 0.001). The spleen-related mortality rate of NOM-obs, SAEs, and surgery was 0%, 0.4%, and 7.2%, respectively. In the SAE subgroup, according to the 2018 AAST-OIS, 234 patients were classified as grade II, n = 3; III, n = 21; IV, n = 111; and V, n = 99, respectively.; and compared with 1994 AST-OIS, 150 patients received a higher grade and the total number of grade IV and V injuries ranged from 96 (41.0%) to 210 (89.7%) (p < 0.0001). On angiography, 202 patients who demonstrated vascular injury and 187 achieved hemostasis after SAE with a 92.6% success rate. Six of the 15 patients failed to SAE preserved the spleen after second embolization with a 95.5% salvage rate.
Conclusions: Our data confirm the superiority of the 2018 AAST-OIS and support the role of SAE in changing the trend of management of BSI.
Keywords: Blunt splenic injury; Contrast extravasation; Pseudoaneurysm; Splenic artery embolization; Splenic salvage rate.
© 2022. The Author(s).
Conflict of interest statement
Drs Being-Chuan Lin, Cheng-Hsien Wu, Yon-Cheong Wong, Huan-Wu Chen, Chen-Ju Fu, Chen-Chih Huang, Chen-Te Wu, and Chi-Hsun Hsieh have no conflicts of interest or financial ties to disclose.
Figures


References
-
- Stassen NA, Bhullar I, Cheng JD, Crandall ML, Friese RS, Guillamondegui OD, Jawa RS, Maung AA, Rohs TJ, Jr, Sangosanya A, Schuster KM, Seamon MJ, Tchorz KM, Zarzuar BL, Kerwin AJ. Selective nonoperative management of blunt splenic injury: an Eastern association for the surgery of Trauma practice management guideline. J Trauma Acute Care Surg. 2012;73:294–300. doi: 10.1097/TA.0b013e3182702afc. - DOI - PubMed
-
- Rowell SE, Biffl WL, Brasel K, Moore EE, Albrecht RA, DeMoya M, Namias N, Schreiber MA, Cohen MJ, Shatz DV, Karmy-Jones R, Moore FA. Western trauma association critical decisions in trauma: management of adult blunt splenic trauma-2016 updates. J Trauma Acute Care Surg. 2017;82:787–793. doi: 10.1097/TA.0000000000001323. - DOI - PubMed
-
- Coccolini F, Montori G, Catena F, Kluger Y, Biffi W, Moore EE, Reva V, Bing C, Bala M, Fugazzola P, Bahouth H, Marzi I, Velmahos G, Ivatury R, Soreide K, Horer T, ten Broek R, Pereira BM, Fraga GP, Inaba K, Kashuk J, Parry N, Masiakos PT, Mylonas KS, Kirkpatrick A, Abu-Zidan F, Gomes CA, Benatti SV, Naidoo N, Salvetti F, Maccatrozzo S, Agnoletti V, Gamberini E, Solaini L, Costanzo A, Celotti A, Tomasoni M, Khokha V, Arvieux C, Napolitano L, Handolin L, Pisano M, Magnone S, Spain DA, Moya M, Davis KA, Angelis ND, Leppaniemi A, Ferrada P, Latifi R, Navarro DC, Otomo Y, Coimbra R, Maier RV, Moore F, Rizoli S, Sakakushev B, Galante JM, Chiara O, Cimbanassi S, Mefire AC, Weber D, Ceresoli M, Peitzman AB, Wehlie L, Sartelli M, Saverio SD, Ansaloni L. Splenic trauma: WSES classification and guidelines for adult and pediatric patients. World J Emerg Surg. 2017;12:40. doi: 10.1186/s13017-017-0151-4. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
