

Cortical symptoms described in emergency calls for patients with suspected large vessel occlusion: a descriptive analysis of 157 emergency calls
- PMID: 35962313
- PMCID: PMC9375237
- DOI: 10.1186/s12873-022-00706-5
Cortical symptoms described in emergency calls for patients with suspected large vessel occlusion: a descriptive analysis of 157 emergency calls
Abstract
Background: Emergency medical dispatchers typically use the dispatch code for suspected stroke when the caller brings up one or more symptoms from the face-arm-speech triad. Paramedics and emergency department physicians are trained to suspect large vessel occlusion stroke when the stroke patient presents with hemiparesis and cortical symptoms: neglect, aphasia, and conjugate eye deviation (CED). We hypothesized that these symptoms could be evident in the emergency call. In this study, we aimed to describe common symptoms mentioned in the emergency calls for paramedic-suspected thrombectomy candidates. Secondly, we wanted to explore how the question about CED arises in the Finnish suspected stroke dispatch protocol. Our third aim was to find out if the symptoms brought up in suspected stroke and non-stroke dispatches differed from each other.
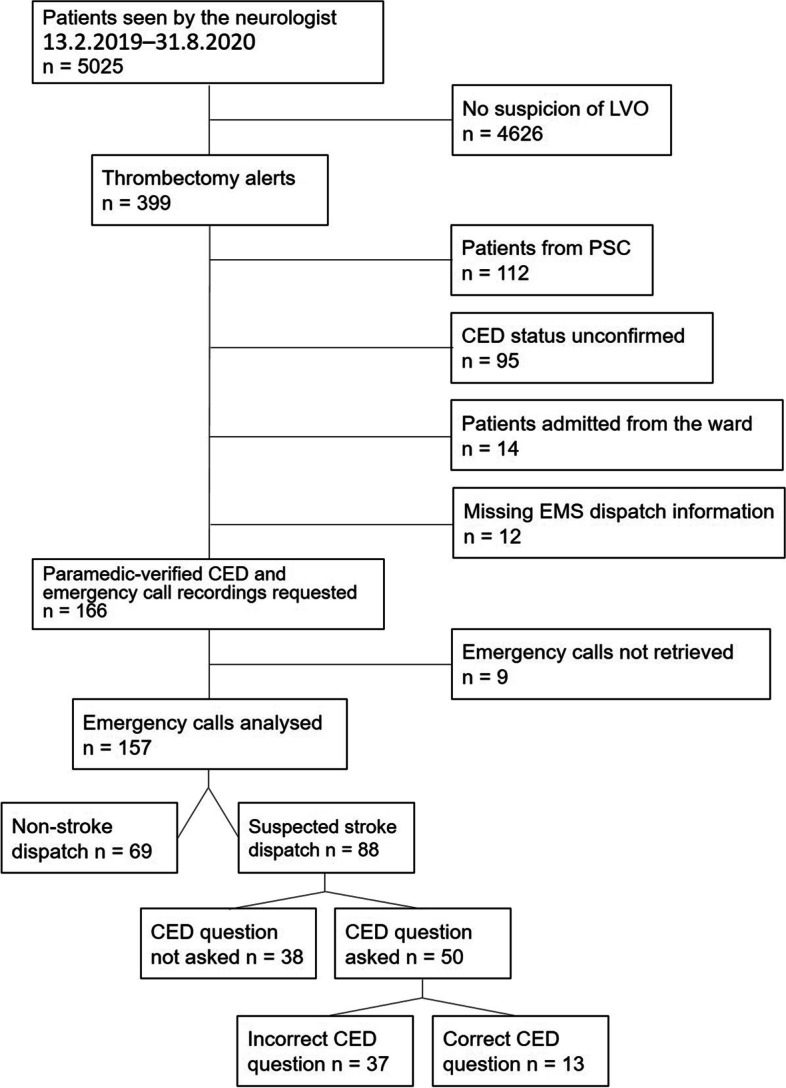
Methods: This was a retrospective study with a descriptive analysis of emergency calls for patients with paramedic-suspected large vessel occlusion stroke. We listened to the emergency calls for 157 patients transported to Tampere University Hospital, a Finnish comprehensive stroke centre. Two researchers listened for symptoms brought up in these calls and filled out a pre-planned case report form.
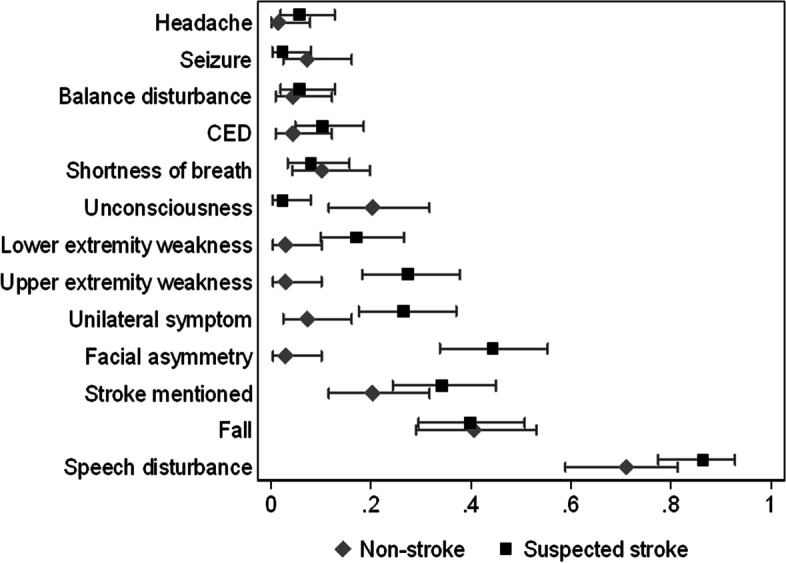
Results: Speech disturbance was the most common symptom brought up in 125 (80%) calls. This was typically described as an inability to speak any words (n = 65, 52% of calls with speech disturbance). Other common symptoms were falling down (n = 63, 40%) and facial asymmetry (n = 41, 26%). Suspicion of stroke was mentioned by 44 (28%) callers. When the caller mentioned unconsciousness the emergency dispatcher tended to use a non-stroke dispatch code. The dispatchers adhered poorly to the protocol and asked about CED in only 57% of suspected stroke dispatches. We found CED in 12 emergency calls and ten of these patients were diagnosed with large vessel occlusion.
Conclusion: In cases where paramedics suspected large vessel occlusion stroke, typical stroke symptoms were described during the emergency call. Speech disturbance was typically described as inability to say anything. It is possible to further develop suspected stroke dispatch protocols to recognize thrombectomy candidates from ischemic cortical signs such as global aphasia and CED.
Keywords: Emergency medical dispatch; Emergency medical services; Large vessel occlusion stroke.
© 2022. The Author(s).
Conflict of interest statement
The authors have no conflicts of interest.
Figures
Similar articles
-
Emergency medical dispatchers' ability to identify large vessel occlusion stroke during emergency calls.Scand J Trauma Resusc Emerg Med. 2021 Jul 19;29(1):97. doi: 10.1186/s13049-021-00914-1. Scand J Trauma Resusc Emerg Med. 2021. PMID: 34281596 Free PMC article.
-
The identification of acute stroke: an analysis of emergency calls.Int J Stroke. 2013 Aug;8(6):408-12. doi: 10.1111/j.1747-4949.2011.00749.x. Epub 2012 Feb 15. Int J Stroke. 2013. PMID: 22335960
-
"Can you send an ambulance please?": a comparison of callers' requests for emergency medical dispatch in non-stroke and stroke calls.Emerg Med J. 2014 Oct;31(e1):e25-8. doi: 10.1136/emermed-2013-202752. Epub 2013 Jul 13. Emerg Med J. 2014. PMID: 23851037
-
Emergency Stroke Calls: Obtaining Rapid Telephone Triage (ESCORTT) – a programme of research to facilitate recognition of stroke by emergency medical dispatchers.Southampton (UK): NIHR Journals Library; 2014 Feb. Southampton (UK): NIHR Journals Library; 2014 Feb. PMID: 25642562 Free Books & Documents. Review.
-
Prehospital Prediction of Large Vessel Occlusion in Suspected Stroke Patients.Curr Atheroscler Rep. 2018 May 21;20(7):34. doi: 10.1007/s11883-018-0734-x. Curr Atheroscler Rep. 2018. PMID: 29781051 Review.
Cited by
-
A hybrid strategy using an ambulance and a helicopter to convey thrombectomy candidates to definite care: a prospective observational study.BMC Emerg Med. 2024 Jan 25;24(1):17. doi: 10.1186/s12873-024-00931-0. BMC Emerg Med. 2024. PMID: 38273239 Free PMC article.
-
Methods for improving the identification of acute stroke during ambulance calls: A scoping review.PLoS One. 2025 Aug 13;20(8):e0327653. doi: 10.1371/journal.pone.0327653. eCollection 2025. PLoS One. 2025. PMID: 40802682 Free PMC article.
-
Impact of the first response unit on prehospital on-scene time among paramedic-suspected stroke patients: a retrospective before-after cohort study in Finland.Scand J Trauma Resusc Emerg Med. 2023 Jun 13;31(1):28. doi: 10.1186/s13049-023-01089-7. Scand J Trauma Resusc Emerg Med. 2023. PMID: 37312108 Free PMC article.
References
-
- Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, et al. American Heart Association Council on epidemiology and prevention: statistics committee and stroke statistics subcommittee. Heart disease and stroke statistics, 2018 update: a report from the American Heart Association. Circulation. 2018;137(12):e67–e492. doi: 10.1161/CIR.0000000000000558. - DOI - PubMed
-
- Boodt N, Compagne KCJ, Dutra BG, Samuels N, Tolhuisen ML, Alves HCBR, et al. Coinvestigators MR CLEAN registry. Stroke etiology and Thrombus computed tomography characteristics in patients with acute ischemic stroke: an MR CLEAN registry substudy. Stroke. 2020;51(6):1727–1735. doi: 10.1161/STROKEAHA.119.027749. - DOI - PubMed
-
- Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, Biller J, et al. Guidelines for the early Management of Patients with Acute Ischemic Stroke (2019 update to the 2018 guidelines): a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50(12):e344–e418. doi: 10.1161/STR.0000000000000211. - DOI - PubMed
-
- Turc G, Bhogal P, Fischer U, Khatri P, Lobotesis K, Mazighi M, et al. European stroke organisation (ESO) and European Society for Minimally Invasive Neurological Therapy (ESMINT) guidelines on mechanical Thrombectomy in acute ischemic stroke. J Neurointerv Surg. 2019;11(6):535–538. doi: 10.1136/neurintsurg-2018-014568. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
