

The diagnosis and treatment in patients with a bipolar fracture-dislocation of the forearm: a retrospective study
- PMID: 35962394
- PMCID: PMC9373530
- DOI: 10.1186/s13018-022-03278-z
The diagnosis and treatment in patients with a bipolar fracture-dislocation of the forearm: a retrospective study
Abstract
Backgrounds: This study aims to investigate the treatment and clinical effect of bipolar fracture-dislocation of the forearm.
Methods: From March 2011 to September 2021, patients with bipolar fracture-dislocation of the forearm admitted to XXX and XXX Hospital were retrospectively analyzed. The timing of rehabilitation depended on the joint stability after the operation. The forearm function was evaluated according to the Anderson forearm function score.
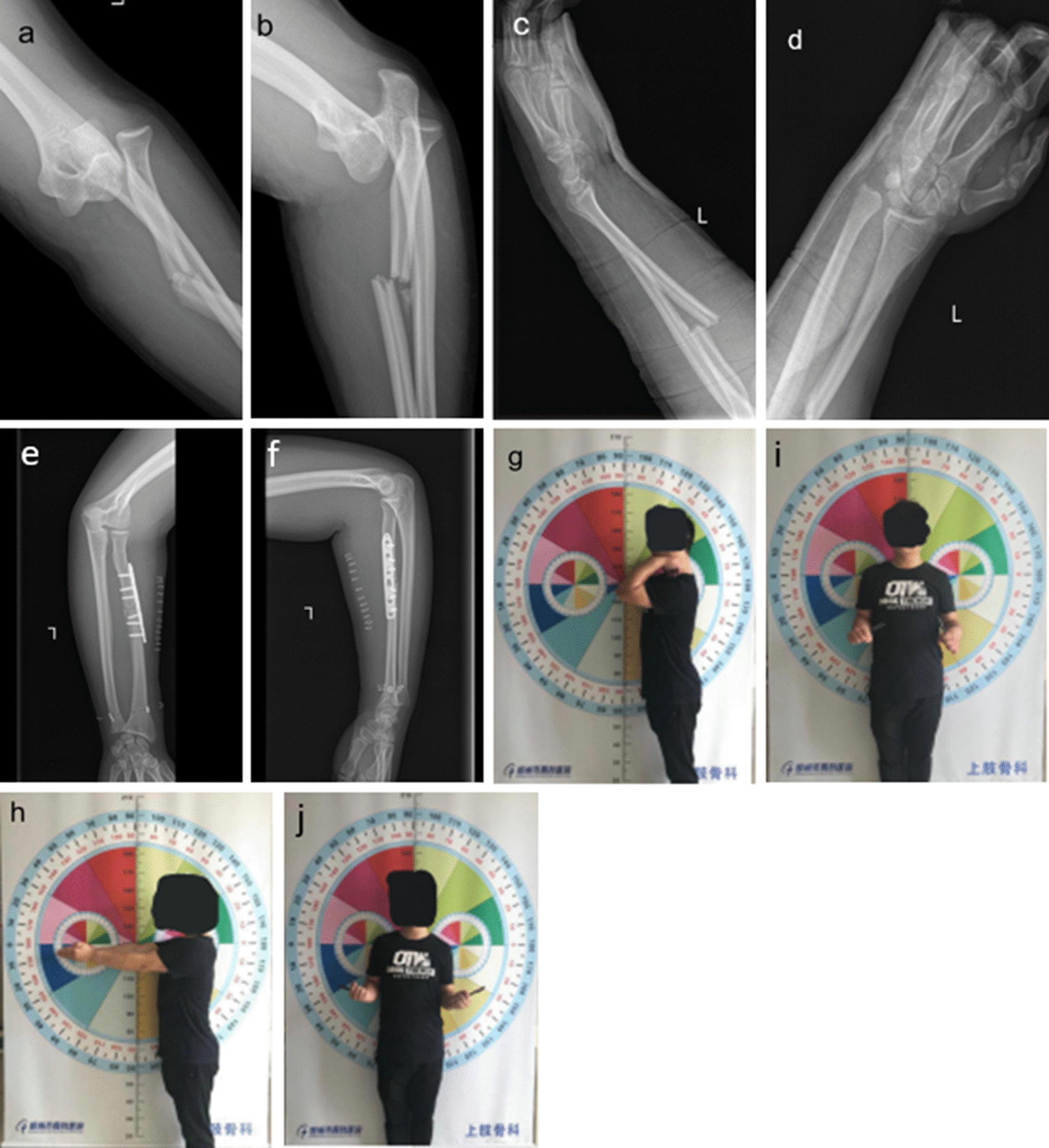
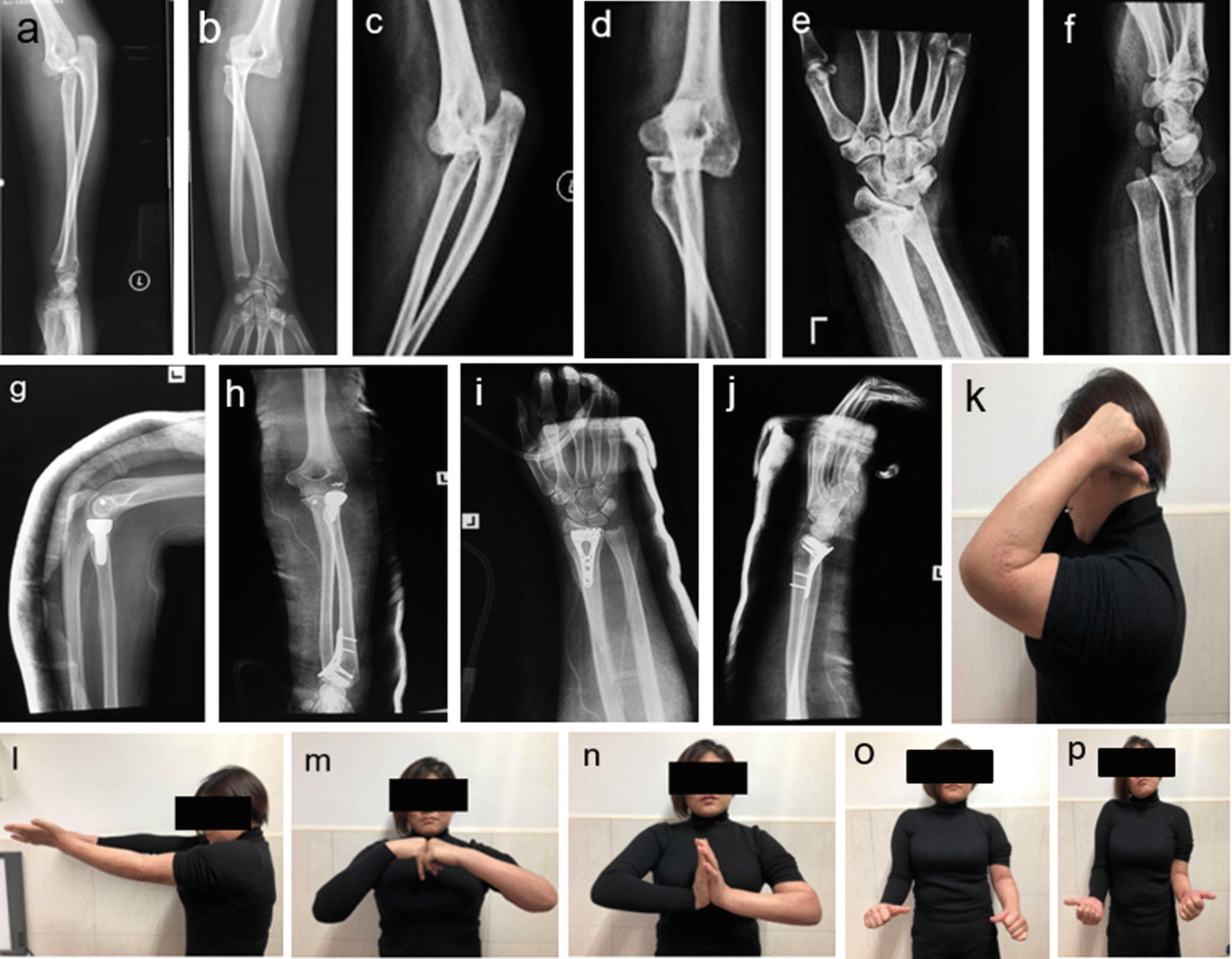
Results: A total of 40 patients who underwent surgical treatment were screened, but only 24 received a minimum of 6 months of follow-ups and were included in the study. Nineteen males and five females were enrolled in the study, with an age range of 18-65 years and an average of 40.4 years. With an average follow-up of 23.6 months (7-62 months), no case was related to functional malformations and infections. The average range of motion of flexion and extension at the elbow was 125.9° (98°-138°), the average range of motion of flexion and extension at the wrist was 144.2° (120°-156°), and the average range of motion of rotation at the forearm was 139.6° (88°-170°). The Anderson's forearm function score of the last follow-up presented: excellent in 16 cases, satisfactory in 6 cases, dissatisfactory in 1 and failure in 1.
Conclusions: Bipolar fracture-dislocation of the forearm always represents high-energy injuries, of which the treatment principle includes complete reduction in distal and proximal dislocations and rehabilitation training as early as possible. Intraoperative fracture fixation follows after a stable reduction in the dislocation.
Keywords: Diagnosis; Elbow dislocations; Forearm injuries; Fractures; High-energy injury.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
[Effectiveness of open reduction and internal fixation for bipolar fracture-dislocation of forearm].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2021 Feb 15;35(2):149-153. doi: 10.7507/1002-1892.202008004. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2021. PMID: 33624465 Free PMC article. Chinese.
-
Terrible triad injuries of the elbow: does the coronoid always need to be fixed?Clin Orthop Relat Res. 2014 Jul;472(7):2084-91. doi: 10.1007/s11999-014-3471-7. Clin Orthop Relat Res. 2014. PMID: 24474322 Free PMC article.
-
[Indication for Radial Head Resection in Traumatology].Acta Chir Orthop Traumatol Cech. 2018;85(3):186-193. Acta Chir Orthop Traumatol Cech. 2018. PMID: 30257777 Czech.
-
Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures. Surgical technique.J Bone Joint Surg Am. 2005 Mar;87 Suppl 1(Pt 1):22-32. doi: 10.2106/JBJS.D.02933. J Bone Joint Surg Am. 2005. PMID: 15743844 Review.
-
Delayed radial head dislocation after radial shaft fracture fixation: a case report and review of the literature.BMC Surg. 2022 Feb 17;22(1):60. doi: 10.1186/s12893-022-01514-1. BMC Surg. 2022. PMID: 35172793 Free PMC article. Review.
References
-
- Monteggia GB. Instituzioni Chirurgische. 2. Milan: Maspero; 1813.
-
- Galeazzi R. Über ein besonderes Syndrom bei Verletzungen im Bereich der Unterarmknochen. Arch Orthop Unfallchir. 1934;35:1557–1562. doi: 10.1007/bf02581917. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
