

Pain levels and patient comfort after lower limb arthroplasty comparing i.v. patient-controlled analgesia, continuous peripheral nerve block and neuraxial analgesia: a retrospective cohort analysis of clinical routine data
- PMID: 35962409
- PMCID: PMC9373442
- DOI: 10.1186/s13018-022-03277-0
Pain levels and patient comfort after lower limb arthroplasty comparing i.v. patient-controlled analgesia, continuous peripheral nerve block and neuraxial analgesia: a retrospective cohort analysis of clinical routine data
Abstract
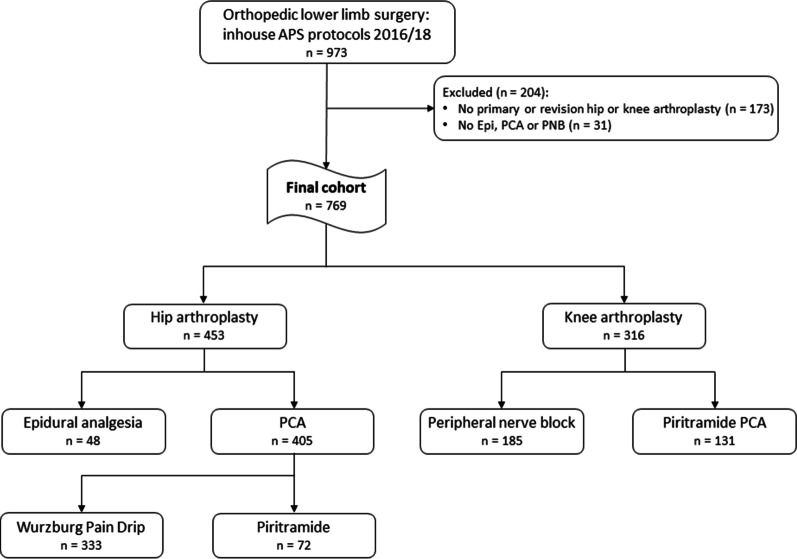
Background: Insufficient pain control after lower limb arthroplasty results in delayed recovery and increased risk for pain chronicization. The ideal kind of analgesia is still discussed controversially. We conducted a retrospective analysis of single-center routine data from a German university hospital, including patients receiving either total hip (THA) or knee arthroplasty (TKA).
Methods: All patients received general anesthesia. Patients undergoing THA received either continuous epidural ropivacaine infusion (0.133%, Epi) or patient-controlled analgesia (PCA) with the Wurzburg Pain Drip (tramadol, metamizole and droperidol, WPD) or with piritramide (Pir). After TKA, patients received either continuous femoral nerve block (ropivacaine 0.2%, PNB) or Pir.
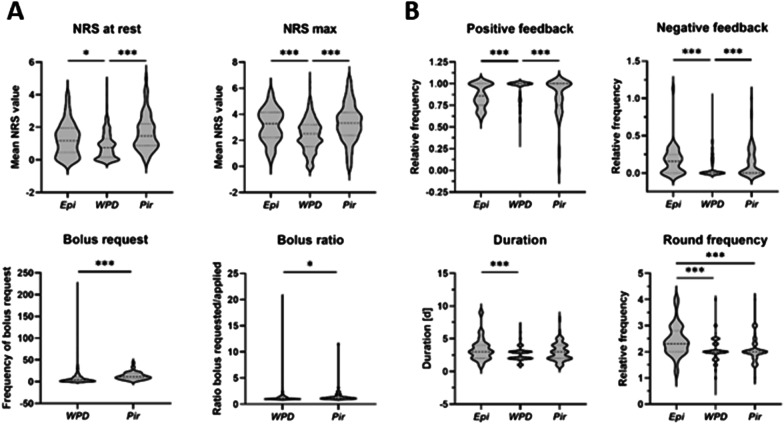
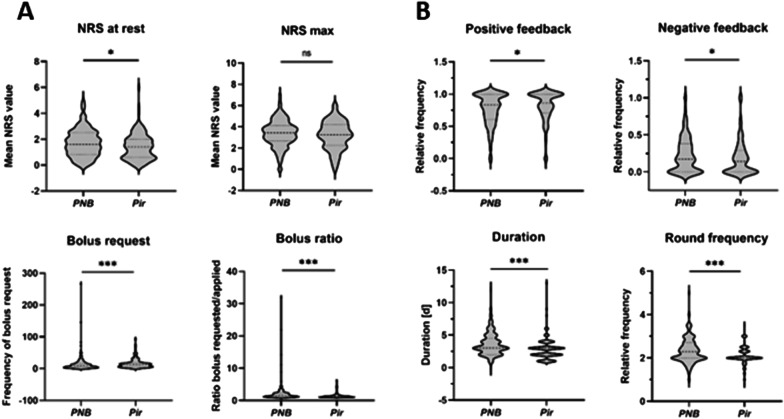
Results: The analyzed cohort comprised 769 cases. Use of WPD after THA (n = 333) resulted in significantly reduced Numeric Rating Scale (NRS) values at rest, compared to Epi (n = 48) and Pir (n = 72) (.75 [IQR 1.14] vs. 1.17 [1.5], p = .02 vs. 1.47 [1.33], p < .0001) as well as maximum NRS scores (2.4 [1.7] vs. 3.29 [1.94], p < .001 vs. 3.32 [1.76], p < .0001). Positive feedback during follow-up visits was significantly increased in patients with a WPD PCA (p < .0001), while negative feedback (senso-motoric weakness/technical problems/nausea/dizziness/constipation) was particularly increased in Epi patients and lowest in those with WPD (p < .0001). After TKA, Pir (n = 131) resulted in significantly reduced NRS values at rest, compared to PNB (n = 185) (1.4 [1.4] vs. 1.6 [1.68], p = .02). Positive feedback was increased in patients with a Pir PCA in comparison with PNB (p = .04), while negative feedback was increased in PNB patients (p = .04). Overall, WPD presented with the lowest rate of any complications (8.7%), followed by Pir (20.2%), PNB (27.6%) and Epi (31.3%) (p < .001).
Conclusions: In the assessed population, the use of a WPD PCA after THA offered better pain control and patient comfort in comparison with continuous epidural or piritramide-based analgesia. After TKA, the use of a Pir PCA provided superior analgesia and a lower complication rate compared to continuous PNB.
Keywords: Hip arthroplasty; Knee arthroplasty; Patient-controlled analgesia; Peripheral nerve block.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
