

Primary stent implantation for bilateral spontaneous cervical ICA dissections with hypoperfusion after 72 h from onset: a case report
- PMID: 35962854
- PMCID: PMC9375808
- DOI: 10.1186/s42155-022-00318-x
Primary stent implantation for bilateral spontaneous cervical ICA dissections with hypoperfusion after 72 h from onset: a case report
Abstract
Background: Spontaneous cervical internal carotid artery dissection (cICAD) is a common cause of stroke in young adults. Endovascular therapy is an indispensable treatment for cICAD in some cases, but it faces great challenges.
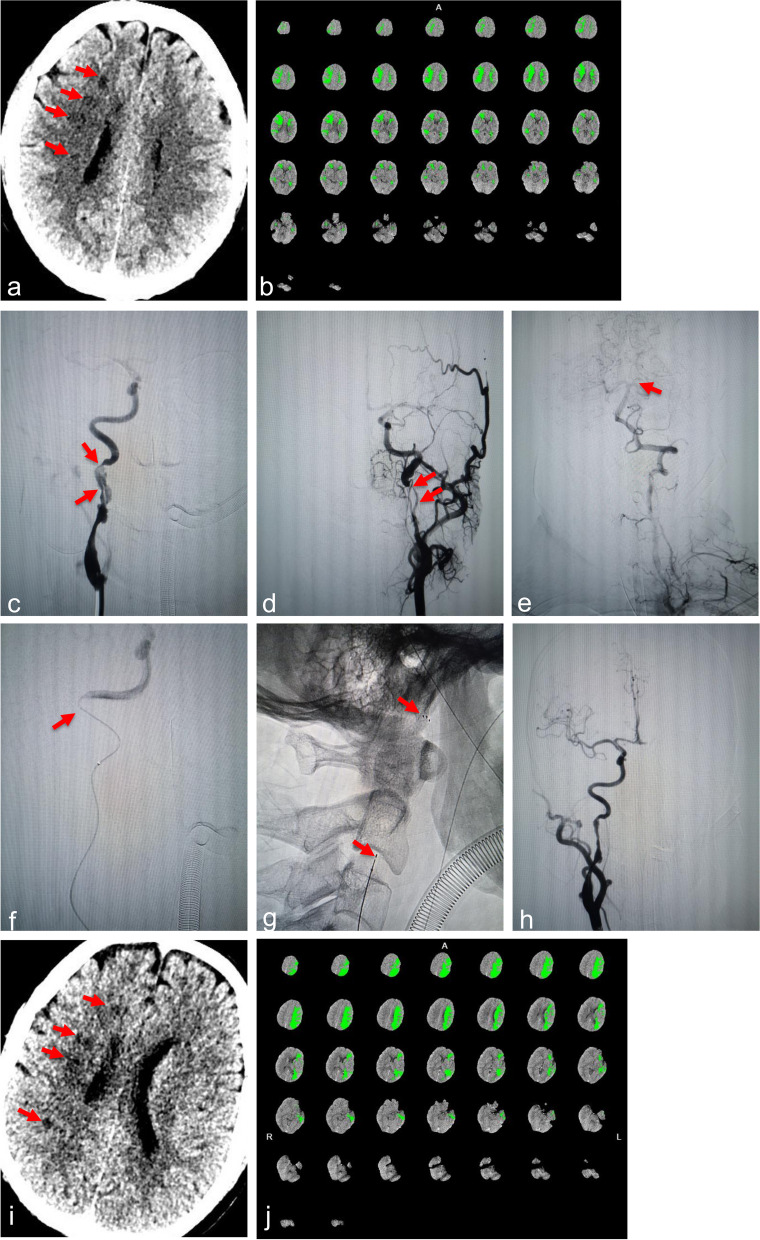
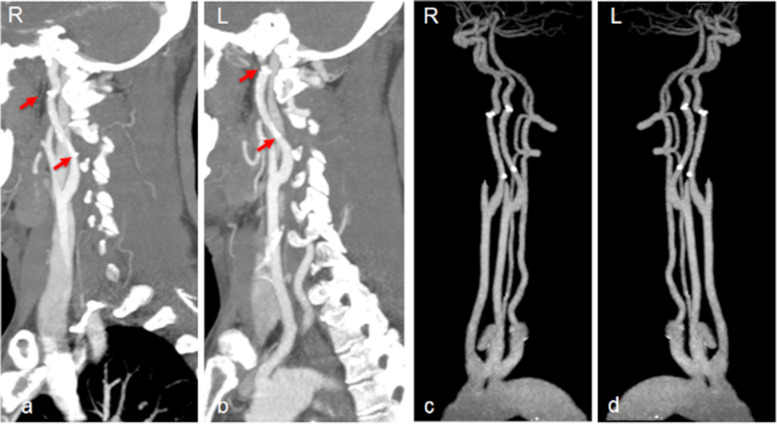
Case presentation: A bilateral spontaneous cICADs with hypoperfusion-related AIS after 72 h from the onset was presented herein. The patient responded well to primary Solitaire stent detachment at the critical flow-limiting site.
Conclusions: Primary stent implantation at the critical flow-limiting site rather than covering the entire dissection may be a therapeutic option in spontaneous cICAD complicated with cerebral hypoperfusion. The Solitaire stent may be a good choice at the acute and subacute stages of cICAD.
Keywords: Acute ischemic stroke; Endovascular treatment; Internal carotid artery; Spontaneous dissection; Stenting.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that we have no competing interests.
Figures

Similar articles
-
Spontaneous Bilateral Cervical Internal Carotid Artery Dissection Treated with Simultaneous Bilateral Carotid Artery Stenting: A Case Report.NMC Case Rep J. 2019 May 25;6(3):71-74. doi: 10.2176/nmccrj.cr.2018-0257. eCollection 2019 Aug. NMC Case Rep J. 2019. PMID: 31417834 Free PMC article.
-
Endovascular Treatment of Spontaneous Intracranial Internal Carotid Dissection in a Young Patient Affected by Systemic Lupus Erythematosus: A Case Report.J Vasc Interv Neurol. 2017 Oct;9(5):1-7. J Vasc Interv Neurol. 2017. PMID: 29163742 Free PMC article.
-
Management of Iatrogenic Internal Carotid Artery Dissection and Middle Cerebral Artery Restenosis during Endovascular Treatment of Acute Stroke: Video Case.Neurosurgery. 2019 Jul 1;85(suppl_1):S70-S71. doi: 10.1093/neuros/nyz043. Neurosurgery. 2019. PMID: 31197330
-
Revascularization of tandem occlusions in acute ischemic stroke: review of the literature and illustrative case.Neurosurg Focus. 2017 Apr;42(4):E15. doi: 10.3171/2017.1.FOCUS16521. Neurosurg Focus. 2017. PMID: 28366063 Review.
-
Ruptured Vertebral Artery Dissecting Aneurysm Concurrent with Spontaneous Cervical Internal Carotid Artery Dissection: A Report of Three Cases and Literature Review.World Neurosurg. 2017 Nov;107:1048.e1-1048.e6. doi: 10.1016/j.wneu.2017.08.016. Epub 2017 Aug 9. World Neurosurg. 2017. PMID: 28803173 Review.
Cited by
-
Initial clinical experience with Xpert-Pro peripheral self-expanding stent system for internal carotid artery dissection: Two case reports.J Interv Med. 2023 Apr 24;6(2):103-106. doi: 10.1016/j.jimed.2023.04.003. eCollection 2023 May. J Interv Med. 2023. PMID: 37409062 Free PMC article.
References
-
- Ansari SA, Kühn AL, Honarmand AR, Khan M, Hurley MC, Potts MB, et al. Emergent Endovascular Management of Long-Segment and Flow-Limiting Carotid Artery Dissections in Acute Ischemic Stroke Intervention with Multiple Tandem Stents. AJNR Am J Neuroradiol. 2017;38:97–104. doi: 10.3174/ajnr.A4965. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous