

Prognostic value of day-of-injury plasma GFAP and UCH-L1 concentrations for predicting functional recovery after traumatic brain injury in patients from the US TRACK-TBI cohort: an observational cohort study
- PMID: 35963263
- PMCID: PMC9462598
- DOI: 10.1016/S1474-4422(22)00256-3
Prognostic value of day-of-injury plasma GFAP and UCH-L1 concentrations for predicting functional recovery after traumatic brain injury in patients from the US TRACK-TBI cohort: an observational cohort study
Abstract
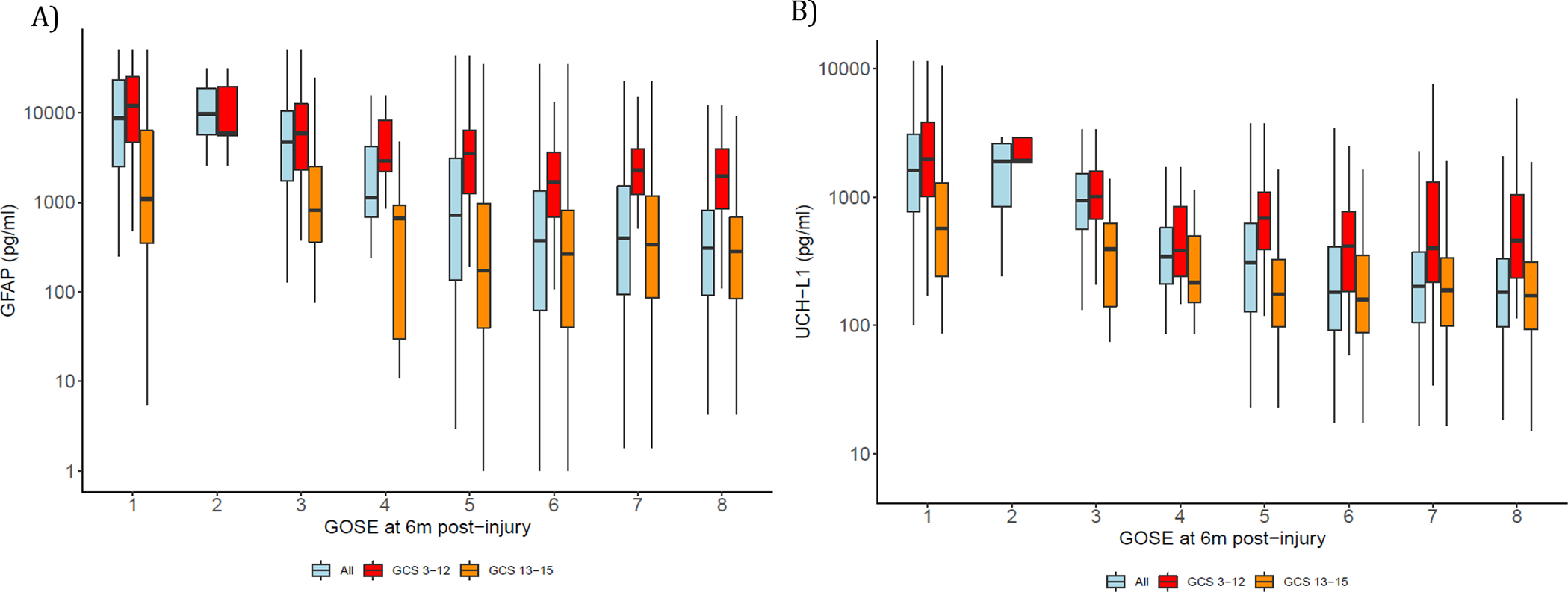
Background: The prognostic value of glial fibrillary acidic protein (GFAP) and ubiquitin C-terminal hydrolase L1 (UCH-L1) as day-of-injury predictors of functional outcome after traumatic brain injury is not well understood. GFAP is a protein found in glial cells and UCH-L1 is found in neurons, and these biomarkers have been cleared to aid in decision making regarding whether brain CT should be performed after traumatic brain injury. We aimed to quantify their prognostic accuracy and investigate whether these biomarkers contribute novel prognostic information to existing clinical models.
Methods: We enrolled patients from the Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI) observational cohort study. TRACK-TBI includes patients 17 years and older who are evaluated for TBI at 18 US level 1 trauma centres. All patients receive head CT at evaluation, have adequate visual acuity and hearing preinjury, and are fluent in either English or Spanish. In our analysis, we included participants aged 17-90 years who had day-of-injury plasma samples for measurement of GFAP and UCH-L1 and completed 6-month assessments for outcome due to traumatic brain injury with the Glasgow Outcome Scale-Extended (GOSE-TBI). Biomarkers were analysed as continuous variables and in quintiles. This study is registered with ClinicalTrials.gov, NCT02119182.
Findings: We enrolled 2552 patients from Feb 26, 2014, to Aug 8, 2018. Of the 1696 participants with brain injury and data available at baseline and at 6 months who were included in the analysis, 120 (7·1%) died (GOSE-TBI=1), 235 (13·9%) had an unfavourable outcome (ie, GOSE-TBI ≤4), 1135 (66·9%) had incomplete recovery (ie, GOSE-TBI <8), and 561 (33·1%) recovered fully (ie, GOSE-TBI=8). The area under the curve (AUC) of GFAP for predicting death at 6 months in all patients was 0·87 (95% CI 0·83-0·91), for unfavourable outcome was 0·86 (0·83-0·89), and for incomplete recovery was 0·62 (0·59-0·64). The corresponding AUCs for UCH-L1 were 0·89 (95% CI 0·86-0·92) for predicting death, 0·86 (0·84-0·89) for unfavourable outcome, and 0·61 (0·59-0·64) for incomplete recovery at 6 months. AUCs were higher for participants with traumatic brain injury and Glasgow Coma Scale (GCS) score of 3-12 than for those with GCS score of 13-15. Among participants with GCS score of 3-12 (n=353), adding GFAP and UCH-L1 (alone or combined) to each of the three International Mission for Prognosis and Analysis of Clinical Trials in traumatic brain injury models significantly increased their AUCs for predicting death (AUC range 0·90-0·94) and unfavourable outcome (AUC range 0·83-0·89). However, among participants with GCS score of 13-15 (n=1297), adding GFAP and UCH-L1 to the UPFRONT study model modestly increased the AUC for predicting incomplete recovery (AUC range 0·69-0·69, p=0·025).
Interpretation: In addition to their known diagnostic value, day-of-injury GFAP and UCH-L1 plasma concentrations have good to excellent prognostic value for predicting death and unfavourable outcome, but not for predicting incomplete recovery at 6 months. These biomarkers contribute the most prognostic information for participants presenting with a GCS score of 3-12.
Funding: US National Institutes of Health, National Institute of Neurologic Disorders and Stroke, US Department of Defense, One Mind, US Army Medical Research and Development Command.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests FKK previously consulted for Abbott Laboratories. FKK and CR have received research funding from Abbott Laboratories. GTM received research funding from a collaboration between Abbott Laboratories and the US Department of Defense. RD-A consulted for MesoScale Discoveries, BrainBox Solutions, and NovaSignal. All other authors and collaborators declare no competing interests.
Figures

Comment in
-
Biomarkers add value to traumatic brain injury prognosis.Lancet Neurol. 2022 Sep;21(9):761-763. doi: 10.1016/S1474-4422(22)00306-4. Lancet Neurol. 2022. PMID: 35963248 No abstract available.
References
-
- Maas AIR, Lingsma HF, Roozenbeek B. Predicting outcome after traumatic brain injury. Handb Clin Neurol 2015; 128: 455–74. - PubMed
-
- Maas AIR, Hukkelhoven CWPM, Marshall LF, Steyerberg EW. Prediction of outcome in traumatic brain injury with computed tomographic characteristics: a comparison between the computed tomographic classification and combinations of computed tomographic predictors. Neurosurgery 2005; 57: 1173–82; discussion 1173–82. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
