

American Association of Clinical Endocrinology Clinical Practice Guideline: Developing a Diabetes Mellitus Comprehensive Care Plan-2022 Update
- PMID: 35963508
- PMCID: PMC10200071
- DOI: 10.1016/j.eprac.2022.08.002
American Association of Clinical Endocrinology Clinical Practice Guideline: Developing a Diabetes Mellitus Comprehensive Care Plan-2022 Update
Erratum in
-
Corrigendum regarding American Association of Clinical Endocrinology Clinical Practice Guideline: Developing a Diabetes Mellitus Comprehensive Care Plan - 2022 Update.Endocr Pract. 2023 Jan;29(1):80-81. doi: 10.1016/j.eprac.2022.12.005. Endocr Pract. 2023. PMID: 36608987 No abstract available.
Abstract
Objective: The objective of this clinical practice guideline is to provide updated and new evidence-based recommendations for the comprehensive care of persons with diabetes mellitus to clinicians, diabetes-care teams, other health care professionals and stakeholders, and individuals with diabetes and their caregivers.
Methods: The American Association of Clinical Endocrinology selected a task force of medical experts and staff who updated and assessed clinical questions and recommendations from the prior 2015 version of this guideline and conducted literature searches for relevant scientific papers published from January 1, 2015, through May 15, 2022. Selected studies from results of literature searches composed the evidence base to update 2015 recommendations as well as to develop new recommendations based on review of clinical evidence, current practice, expertise, and consensus, according to established American Association of Clinical Endocrinology protocol for guideline development.
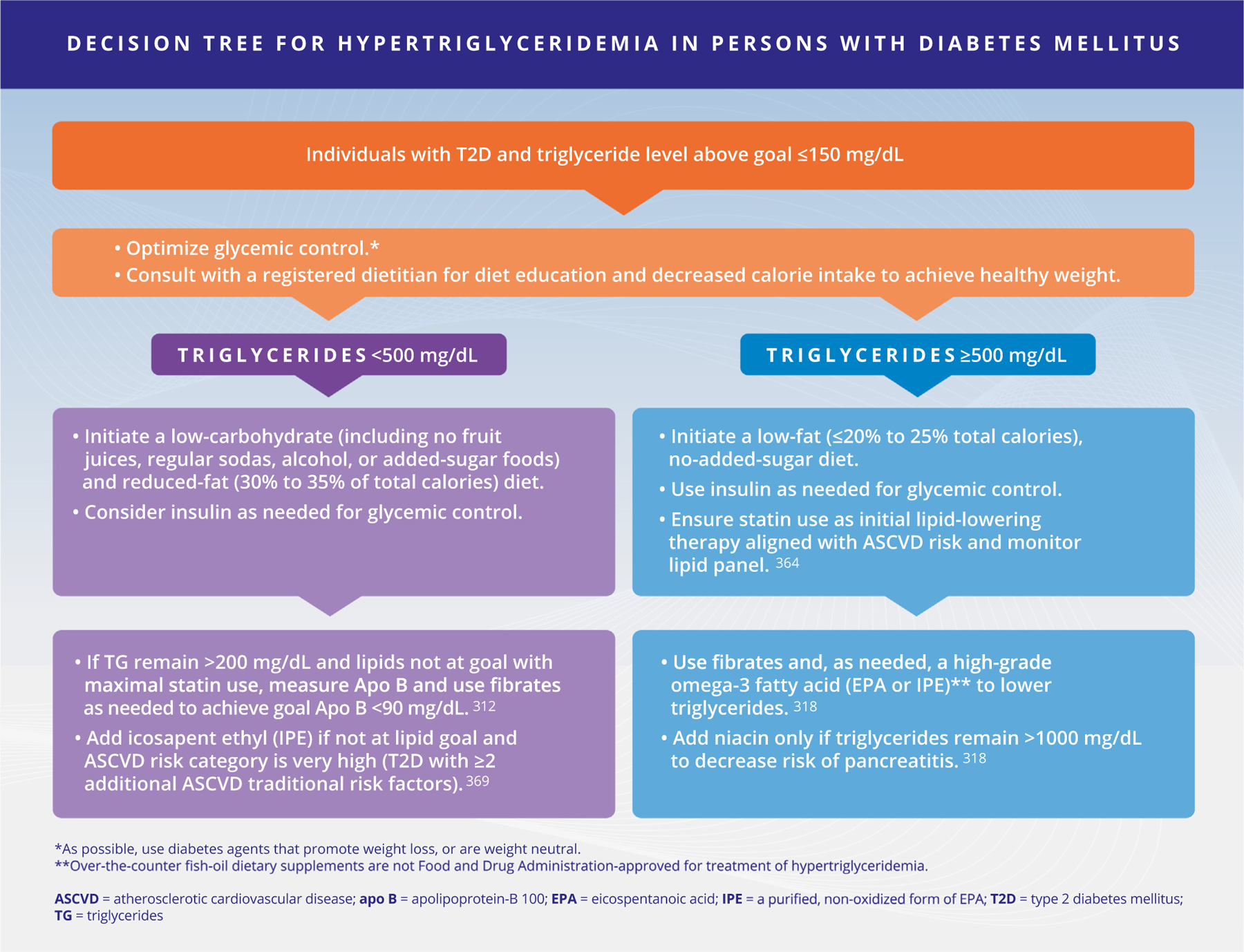
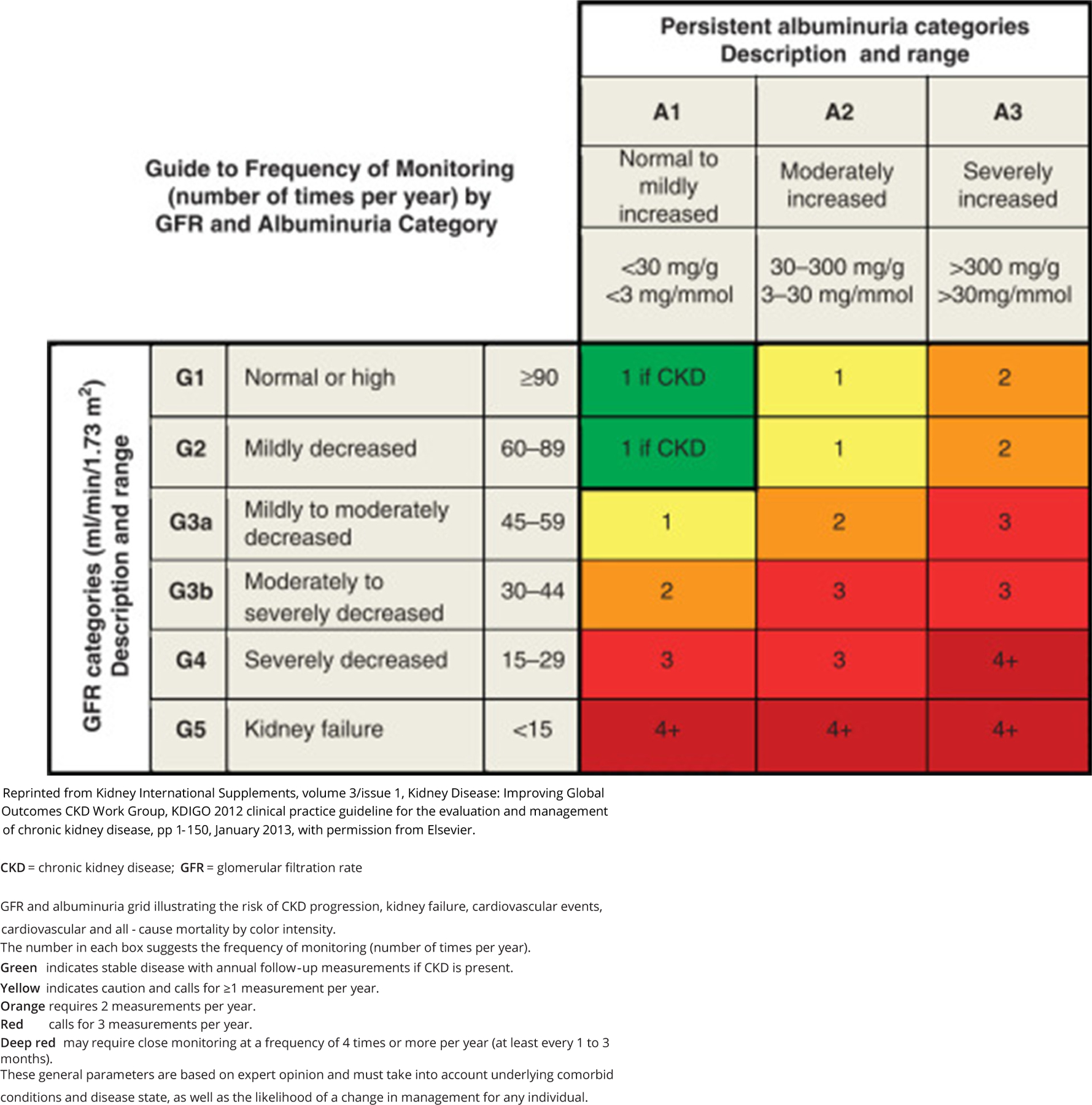
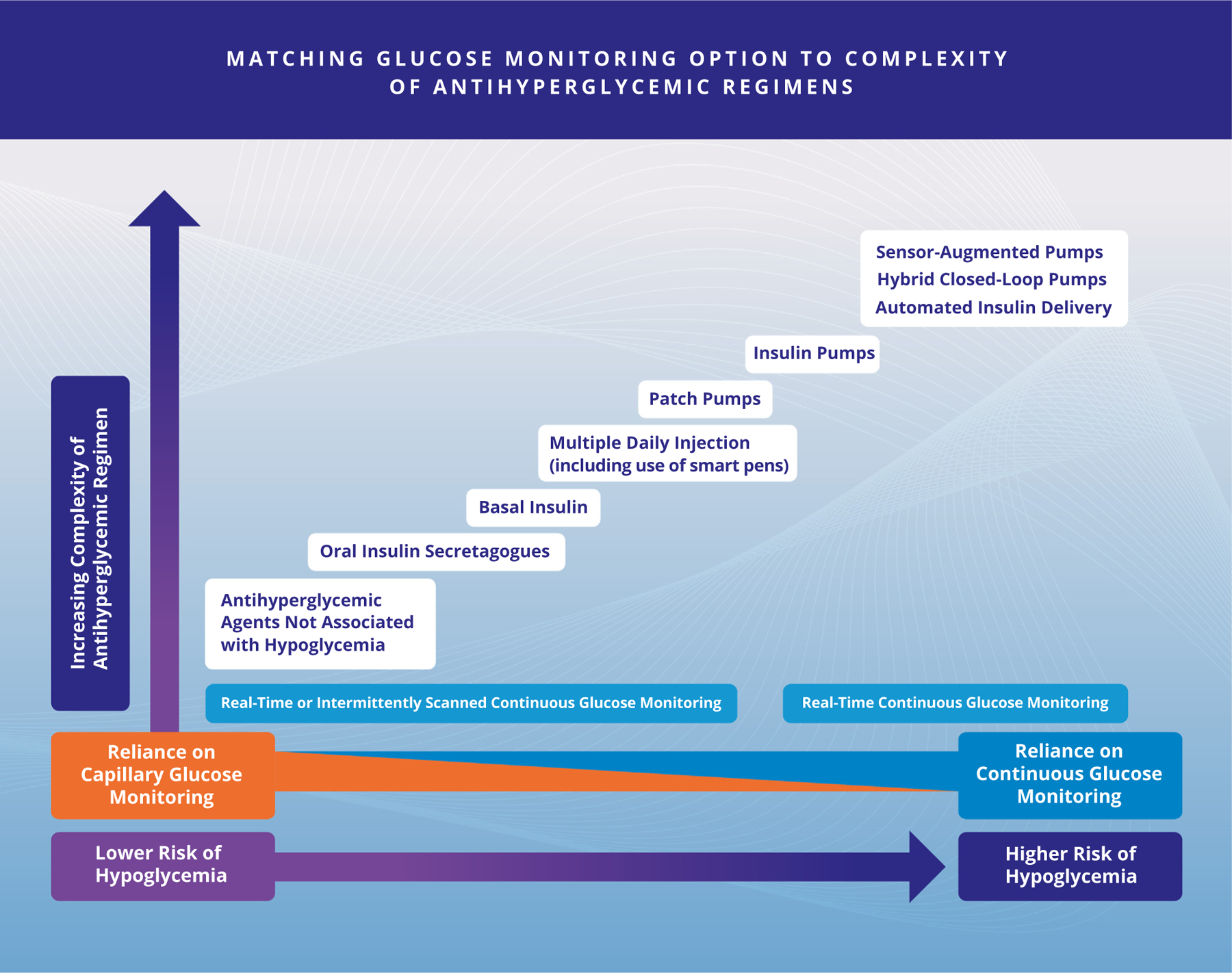
Results: This guideline includes 170 updated and new evidence-based clinical practice recommendations for the comprehensive care of persons with diabetes. Recommendations are divided into four sections: (1) screening, diagnosis, glycemic targets, and glycemic monitoring; (2) comorbidities and complications, including obesity and management with lifestyle, nutrition, and bariatric surgery, hypertension, dyslipidemia, retinopathy, neuropathy, diabetic kidney disease, and cardiovascular disease; (3) management of prediabetes, type 2 diabetes with antihyperglycemic pharmacotherapy and glycemic targets, type 1 diabetes with insulin therapy, hypoglycemia, hospitalized persons, and women with diabetes in pregnancy; (4) education and new topics regarding diabetes and infertility, nutritional supplements, secondary diabetes, social determinants of health, and virtual care, as well as updated recommendations on cancer risk, nonpharmacologic components of pediatric care plans, depression, education and team approach, occupational risk, role of sleep medicine, and vaccinations in persons with diabetes.
Conclusions: This updated clinical practice guideline provides evidence-based recommendations to assist with person-centered, team-based clinical decision-making to improve the care of persons with diabetes mellitus.
Keywords: antihyperglycemic medications; atherosclerotic cardiovascular disease; cardiovascular diseases; diabetes; diabetes mellitus; diabetes mellitus, type 1; diabetes mellitus, type 2; diabetic nephropathies; diabetic neuropathies; diabetic retinopathy; dyslipidemias; gestational; guideline; hospitalization; hypertension; hypoglycemia; infertility; interdisciplinary communication; metabolic syndrome; obesity; occupations; prediabetic state; pregnancy; secondary diabetes; sleep apnea syndromes; telemedicine; vaccination.
Copyright © 2022 AACE. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosures and Conflicts of Interest Policy
The Task Force was empaneled in accordance with AACE’s Conflict of Interest (COI) Policy and approved by the AACE COI Subcommittee. All members of the expert Task Force completed AACE’s disclosure form regarding any multiplicities of interests related to commercial and direct financial relationships within the preceding 12 months with companies that develop products connected with endocrine disorders. Categories for disclosure include employment, stock or other ownership, direct financial relationships (eg, speaker or consultant), research funding, authorship or panel involvement on a guideline related to an overlapping topic, or other situations related to a perceived COI. The AACE COI Subcommittee reviewed these disclosures against an AACE-approved list of affected companies for this guideline and reached consensus regarding members who could serve on the Task Force in the nonconflicted majority, those who could serve in the conflicted minority with management strategy, and those who were disqualified from serving on the Task Force. The AACE CPG Oversight Committee reviewed and approved the AACE COI Subcommittee’s decisions regarding manageable COI and empanelment. Members of this Task Force were reminded to update potential disclosures if new potential conflicts arose during their appointments and to verifycurrency of disclosures. AACE made every effort to minimize the potential for conflicts of interest that could influence the recommendations of this CPG.
Figures



References
-
- Handelsman Y, Bloomgarden ZT, Grunberger G, et al. American Association of Clinical Endocrinologists and American College of Endocrinology - clinical practice guidelines for developing a diabetes mellitus comprehensive care plan - 2015. Endocr Pract 2015;21(suppl 1):1–87. 10.4158/EP15672. GL [EL 4; NE]. - DOI - PMC - PubMed
-
- Mechanick JI, Pessah-Pollack R, Camacho P, et al. American Association of Clinical Endocrinologists and American College of Endocrinology protocol for standardized production of clinical practice guidelines, algorithms, and checklists - 2017 update. Endocr Pract 2017;23(8):1006–1021. 10.4158/EP171866. GL [EL 4; NE]. - DOI - PubMed
