

Bedside assessment of left atrial pressure in critical care: a multifaceted gem
- PMID: 35964098
- PMCID: PMC9375940
- DOI: 10.1186/s13054-022-04115-9
Bedside assessment of left atrial pressure in critical care: a multifaceted gem
Abstract
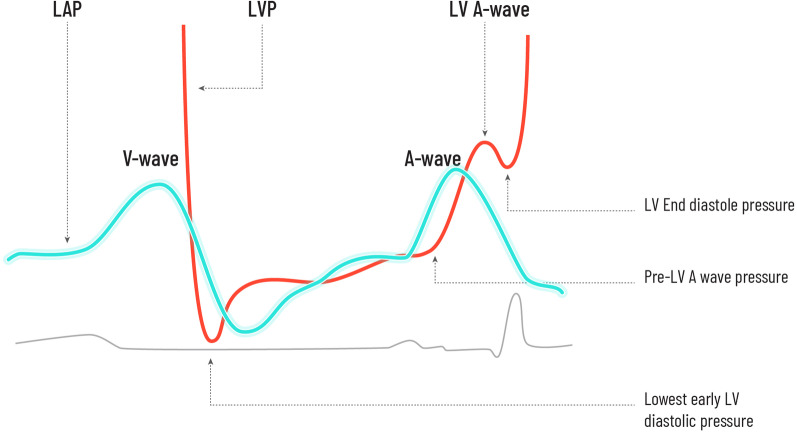
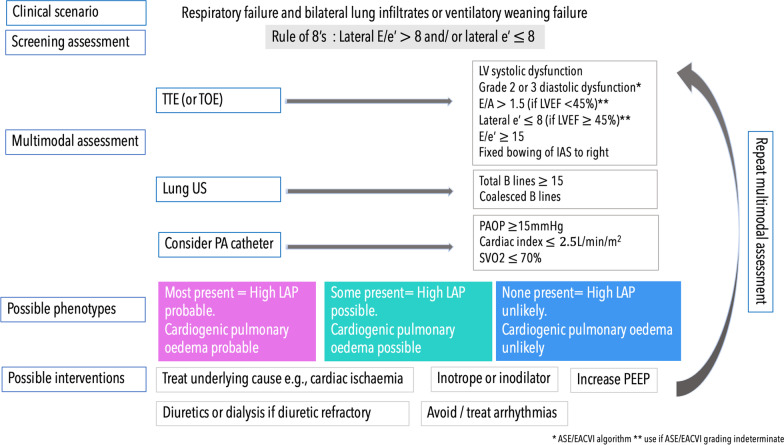
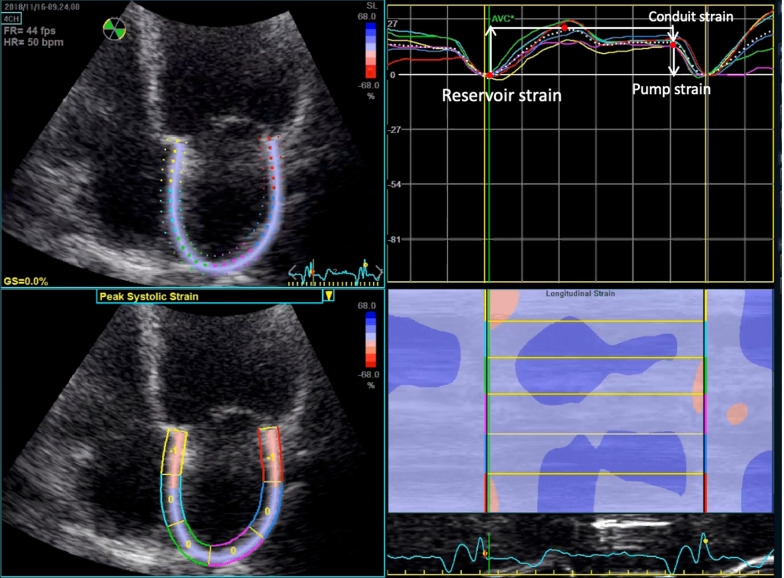
Evaluating left atrial pressure (LAP) solely from the left ventricular preload perspective is a restrained approach. Accurate assessment of LAP is particularly relevant when pulmonary congestion and/or right heart dysfunction are present since it is the pressure most closely related to pulmonary venous pressure and thus pulmonary haemodynamic load. Amalgamation of LAP measurement into assessment of the 'transpulmonary circuit' may have a particular role in differentiating cardiac failure phenotypes in critical care. Most of the literature in this area involves cardiology patients, and gaps of knowledge in application to the bedside of the critically ill patient remain significant. Explored in this review is an overview of left atrial physiology, invasive and non-invasive methods of LAP measurement and their potential clinical application.
Keywords: Cardiac phenotypes; Left atrial physiology; Left atrial pressure; Left atrial strain; Left ventricular end-diastolic pressure; Right ventricular–pulmonary circuit; Transpulmonary circuit.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




References
-
- Sanfilippo F, Corredor C, Arcadipane A, Landesberg G, Vieillard-Baron A, Cecconi M, et al. Tissue Doppler assessment of diastolic function and relationship with mortality in critically ill septic patients: a systematic review and meta-analysis. Br J Anaesth. 2017;119(4):583–594. doi: 10.1093/bja/aex254. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
