

Patterns and determinants of adherence to resistance and endurance training during cancer treatment in the Phys-Can RCT
- PMID: 35964124
- PMCID: PMC9375909
- DOI: 10.1186/s13102-022-00548-5
Patterns and determinants of adherence to resistance and endurance training during cancer treatment in the Phys-Can RCT
Abstract
Background: Knowledge regarding adherence is necessary to improve the specificity of exercise interventions during cancer treatment. We aimed to determine adherence to resistance and endurance training interventions in parallel; identify subgroups with similar adherence characteristics; and examine determinants of these subgroups.
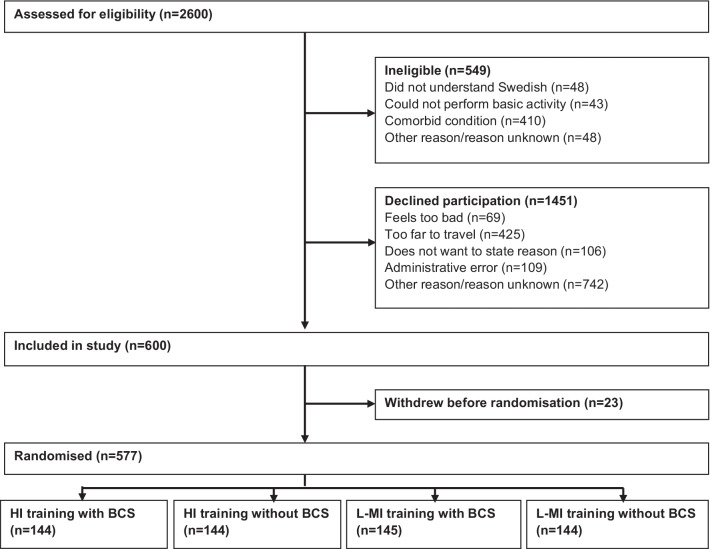
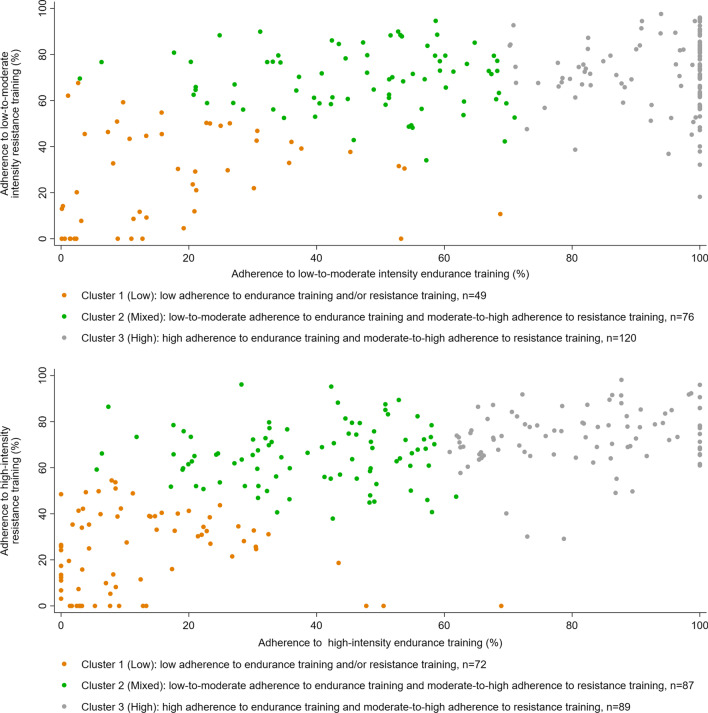
Methods: In the Phys-Can randomised controlled trial, participants (n = 577, 81% women, mean(SD) age 59(12) years, and 50% with BMI ≥ 25 kg/m2) starting (neo-) adjuvant treatment for breast, colorectal or prostate cancer were randomized to 6-month of high (HI) or low-to-moderate intensity (LMI) supervised, group-based resistance training and individual home-based endurance training, with or without behavior change support. Adherence was calculated as performed exercise volume as a proportion of prescribed exercise volume (0-100%), overall (HI and LMI groups) and for frequency, intensity, type and time (FITT principles) (HI group). Adherence to resistance training was plotted against adherence to endurance training overall and for each FITT principle. K-means cluster analysis was used to identify subgroups with similar adherence characteristics. Potential determinants of subgroup membership were examined using multinomial logistic regression.
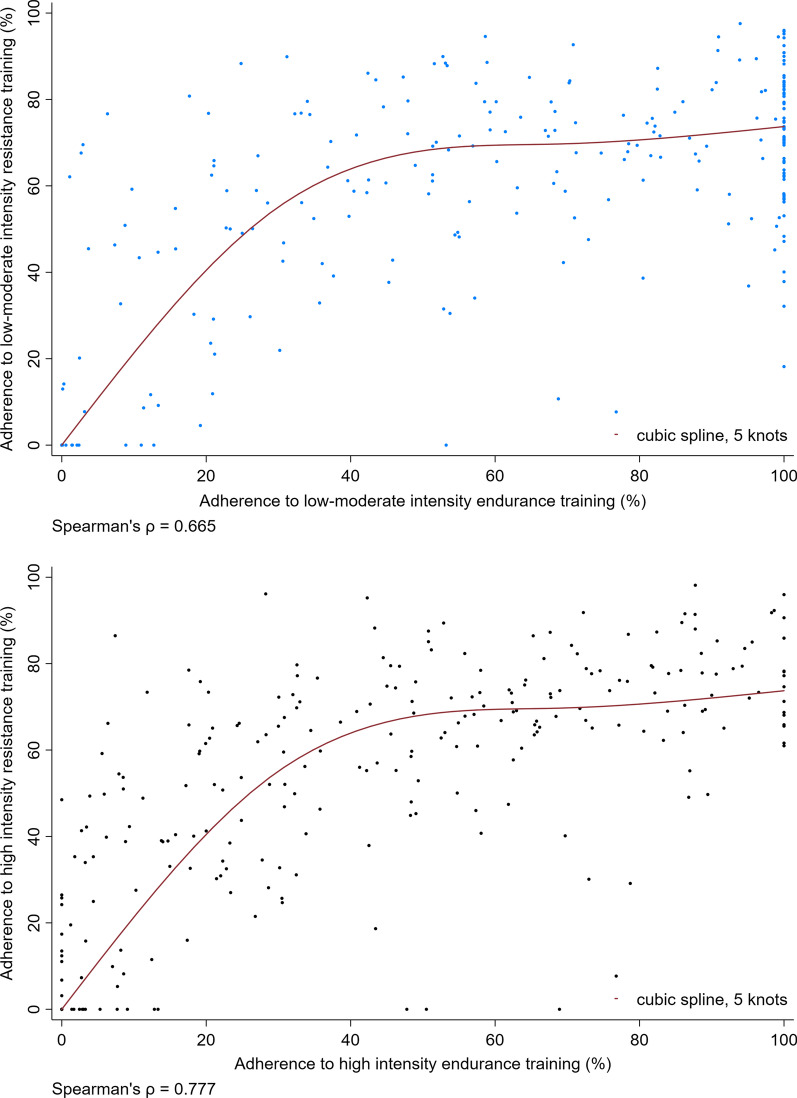
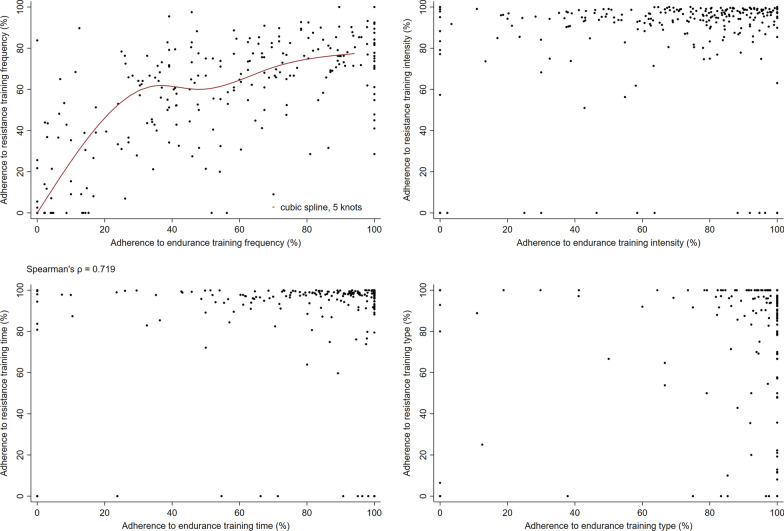
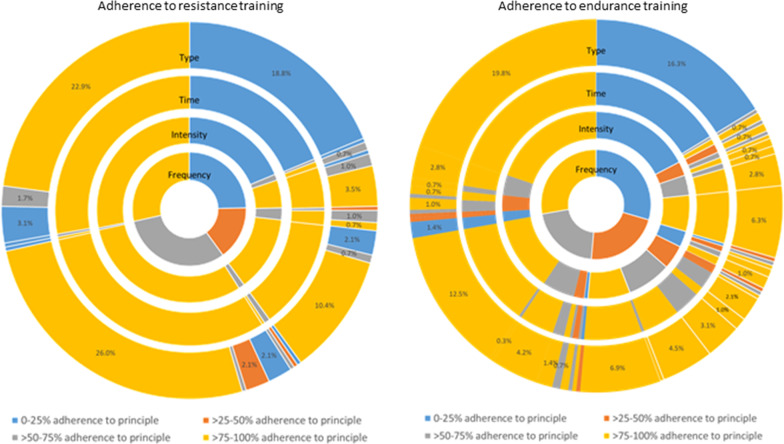
Results: We found a positive curvilinear correlation between adherence to resistance and endurance training overall. A similar correlation was seen for adherence to frequency of resistance vs. endurance training in the HI group. In the HI group, adherence to resistance training intensity and time was > 80% for almost all participants. For endurance training adherence ranged from 0 to 100% for each of the FITT principles. Three clusters were identified, representing low, mixed, and high adherence to resistance and endurance training overall. Participants with higher age (Relative risk ratio [95% CI]; LMI: 0.86[0.77-0.96], HI: 0.83[0.74-0.93]), no behaviour change support (LMI: 0.11[0.02-0.56], HI: 0.20[0.05-0.85]), higher cardiorespiratory fitness (LMI: 0.81[0.69-0.94], HI: 0.80[0.69-0.92]), more fatigue (according to the reduced activity subscale of the MFI questionnaire) (LMI: 0.48[0.31-0.73], HI: 0.69[0.52-0.93]) or higher quality of life (LMI: 0.95[0.90-1.00], HI: 0.93[0.88-0.98]) were less likely to be in the low than the high adherence cluster whether randomised to LMI or HI training. Other determinants were specific to those randomised to LMI or HI training.
Conclusions: In an exercise intervention during cancer treatment, adherence to resistance and endurance training were positively correlated. Personalisation of interventions and additional support for some subgroups of participants may improve adherence. Trial registration NCT02473003 (clinicaltrials.gov, Registered 16/06/2015).
Keywords: Adherence; Cancer; Determinants; Endurance training; Exercise; FITT principles; Patterns; Resistance training.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Exploring Moderators of the Effect of High vs. Low-to-Moderate Intensity Exercise on Cardiorespiratory Fitness During Breast Cancer Treatment - Analyses of a Subsample From the Phys-Can RCT.Front Sports Act Living. 2022 Jul 12;4:902124. doi: 10.3389/fspor.2022.902124. eCollection 2022. Front Sports Act Living. 2022. PMID: 35903402 Free PMC article.
-
Exercise Adherence and Effect of Self-Regulatory Behavior Change Techniques in Patients Undergoing Curative Cancer Treatment: Secondary Analysis from the Phys-Can Randomized Controlled Trial.Integr Cancer Ther. 2020 Jan-Dec;19:1534735420946834. doi: 10.1177/1534735420946834. Integr Cancer Ther. 2020. PMID: 32909467 Free PMC article. Clinical Trial.
-
Randomized controlled trial of the effects of high intensity and low-to-moderate intensity exercise on physical fitness and fatigue in cancer survivors: results of the Resistance and Endurance exercise After ChemoTherapy (REACT) study.BMC Med. 2015 Oct 29;13:275. doi: 10.1186/s12916-015-0513-2. BMC Med. 2015. PMID: 26515383 Free PMC article. Clinical Trial.
-
Attention to principles of exercise training: an updated systematic review of randomized controlled trials in cancers other than breast and prostate.BMC Cancer. 2021 Nov 5;21(1):1179. doi: 10.1186/s12885-021-08701-y. BMC Cancer. 2021. PMID: 34740332 Free PMC article.
-
Attention to the Principles of Exercise Training in Exercise Studies of Persons With Lung Cancer: A Systematic Review.J Aging Phys Act. 2021 May 7;29(6):1042-1052. doi: 10.1123/japa.2020-0269. J Aging Phys Act. 2021. PMID: 33963092
Cited by
-
Comparative Efficacy of Different Exercise Therapies for Cardiorespiratory Fitness in Breast Cancer Survivors: A Systematic Review and Bayesian Network Meta-analysis.Sports Med Open. 2025 Jun 8;11(1):67. doi: 10.1186/s40798-025-00872-3. Sports Med Open. 2025. PMID: 40483630 Free PMC article.
References
Associated data
LinkOut - more resources
Full Text Sources
Medical
