

Optimizing treatment management of trastuzumab deruxtecan in clinical practice of breast cancer
- PMID: 35964548
- PMCID: PMC9375150
- DOI: 10.1016/j.esmoop.2022.100553
Optimizing treatment management of trastuzumab deruxtecan in clinical practice of breast cancer
Abstract
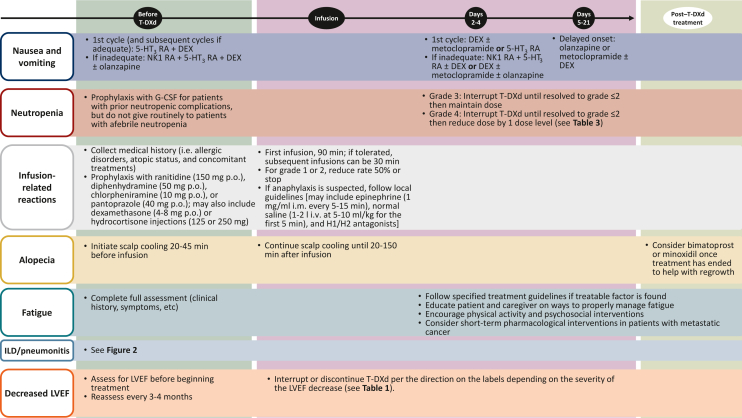
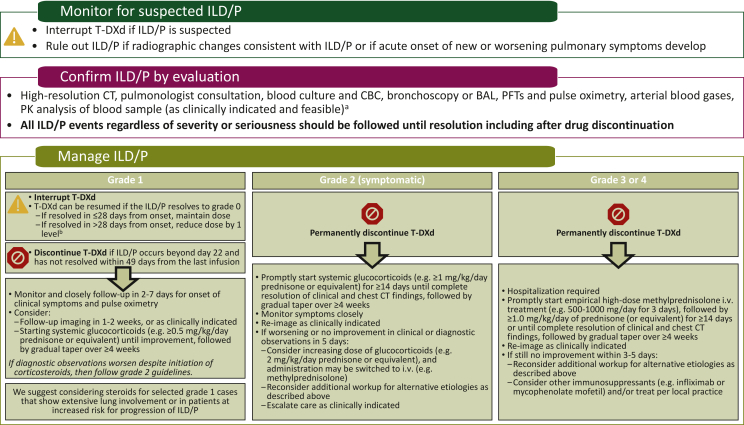
Introduction: The antibody-drug conjugate trastuzumab deruxtecan (T-DXd) targets human epidermal growth factor receptor 2 (HER2) and has been evaluated in patients with HER2-positive unresectable/metastatic breast cancer in the phase II DESTINY-Breast01 trial (NCT03248492; DS8201-A-U201) and the randomized phase III DESTINY-Breast03 trial (NCT03529110; DS8201-A-U302). Approximately 20 additional studies are ongoing in breast cancer, including HER2-low breast cancer, and other solid tumor types within the DESTINY trial program. T-DXd has demonstrated a generally manageable safety profile, with low-grade hematologic and gastrointestinal adverse events (AEs) among the most common; interstitial lung disease (ILD)/pneumonitis has been observed in patients receiving T-DXd and can be severe. This review discusses the management of common AEs and AEs of special interest in patients with HER2-positive unresectable/metastatic breast cancer, including nausea and vomiting, neutropenia, infusion-related reactions, alopecia, fatigue, ILD/pneumonitis, and left ventricular dysfunction.
Methods: Expert opinions, institutional protocols, and strategies to help optimize AE management and maximize the potential benefits of T-DXd in patients with breast cancer from five oncologists treating patients with T-DXd in North America and Europe are discussed.
Results: Prophylaxis for nausea and vomiting and proactive management of ILD/pneumonitis are especially important in treating patients with T-DXd. Management strategies for other T-DXd-related AEs of interest (e.g. neutropenia, infusion-related reactions, alopecia, fatigue, and left ventricular dysfunction) are also discussed.
Conclusions: This review provides context for understanding the usage, monitoring, and management practices of other health care providers and institutions with experience using T-DXd to help with safe and effective management of T-DXd-related AEs, particularly since the duration of T-DXd treatment may be quite long. Proper management of T-DXd-related AEs will allow optimal exposure and benefit from T-DXd and will help avoid premature discontinuation or improper dose reductions.
Keywords: adverse event; breast cancer; interstitial lung disease; nausea; trastuzumab deruxtecan; vomiting.
Copyright © 2022 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Disclosure All authors received nonfinancial support (assistance with manuscript preparation) from ArticulateScience LLC funded by AstraZeneca. Additional disclosures are as follows: HSR reports travel expenses from Pfizer, Puma Biotechnology, Mylan, Amgen, Daiichi Sankyo, Merck, Novartis, and OBI Pharma; and research funding from MacroGenics, OBI Pharma, Eisai, Pfizer, Novartis, Lilly, Genentech, Merck, Immunomedics, Odonate Therapeutics, Daiichi Sankyo, and Seattle Genetics. GB reports consulting fees from Roche, AstraZeneca, Merck Sharp & Dohme (MSD), Daiichi Sankyo, Gilead, and Sanofi; honoraria from Roche, AstraZeneca, Daiichi Sankyo, Lilly, MSD, Chugai, Eisai, Gilead, and Seagen; travel from Roche, Pfizer, MSD, Chugai, and Novartis; and data safety monitoring or advisory boards from Roche, Pfizer, AstraZeneca, Lilly, Novartis, Amgen, MSD, Chugai, Daiichi Sankyo, Eisai, Gilead, Seagen, and Exact Science. JC reports consulting or advisory roles for Roche, Celgene, Cellestia, AstraZeneca, Biothera Pharmaceutical, Merus, Seattle Genetics, Daiichi Sankyo, Erytech, Athenex, Polyphor, Lilly, Servier, MSD, GlaxoSmithKline, Leuko, Bioasis, Clovis Oncology, Boehringer Ingelheim, and Kyowa Kirin; honoraria from Roche, Novartis, Celgene, Eisai, Pfizer, Samsung Bioepis, Lilly, MSD, and Daiichi Sankyo; research funding from Roche, Ariad Pharmaceuticals, AstraZeneca, Baxalta GmbH/Servier Affaires, Bayer Healthcare, Eisai, F. Hoffmann-La Roche, Guardant Health, MSD, Pfizer, Piqur Therapeutics, Puma C, and Queen Mary University of London; stock, patents, and intellectual property from MedSIR; and travel expenses from Roche, Novartis, Eisai, Pfizer, and Daiichi Sankyo. JWH reports fees for advisory boards, lectures, presentations, speakers bureau, and educational events from AstraZeneca, Gilead, Pfizer, Lilly, and Novartis. MU reports fees for advisory boards, speakers bureau, and travel expenses from AbbVie, Amgen GmbH München, AstraZeneca, Bristol Myers Squibb, Celgene GmbH München, Janssen Cilag, Johnson & Johnson, Lilly Deutschland, Lilly International, MSD, Mundipharma, Myriad Genetics GmbH Zürich, Odonate, Pfizer GmbH Berlin, Puma Biotechnology, Riemser, Roche Pharma AG, Sanofi Aventis Deutschland GmbH, Sividon Diagnostics Köln, and Teva Pharmaceuticals Ltd.
Figures
References
-
- Doi T., Shitara K., Naito Y., et al. Safety, pharmacokinetics, and antitumour activity of trastuzumab deruxtecan (DS-8201), a HER2-targeting antibody-drug conjugate, in patients with advanced breast and gastric or gastro-oesophageal tumours: a phase 1 dose-escalation study. Lancet Oncol. 2017;18(11):1512–1522. - PubMed
-
- Ogitani Y., Aida T., Hagihara K., et al. DS-8201a, a novel HER2-targeting ADC with a novel DNA topoisomerase I inhibitor, demonstrates a promising antitumor efficacy with differentiation from T-DM1. Clin Cancer Res. 2016;22(20):5097–5108. - PubMed
-
- Nakada T., Sugihara K., Jikoh T., Abe Y., Agatsuma T. The latest research and development into the antibody-drug conjugate, [fam-] trastuzumab deruxtecan (DS-8201a), for HER2 cancer therapy. Chem Pharm Bull (Tokyo) 2019;67(3):173–185. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
