

Human papillomavirus vaccine effectiveness by number of doses: Updated systematic review of data from national immunization programs
- PMID: 35965239
- PMCID: PMC9768820
- DOI: 10.1016/j.vaccine.2022.06.065
Human papillomavirus vaccine effectiveness by number of doses: Updated systematic review of data from national immunization programs
Abstract
Background: Human papillomavirus (HPV) vaccines were first licensed as a three-dose series. Two doses are now widely recommended in some age groups; there are data suggesting high efficacy with one dose. We updated a systematic literature review of HPV vaccine effectiveness by number of doses in observational studies.
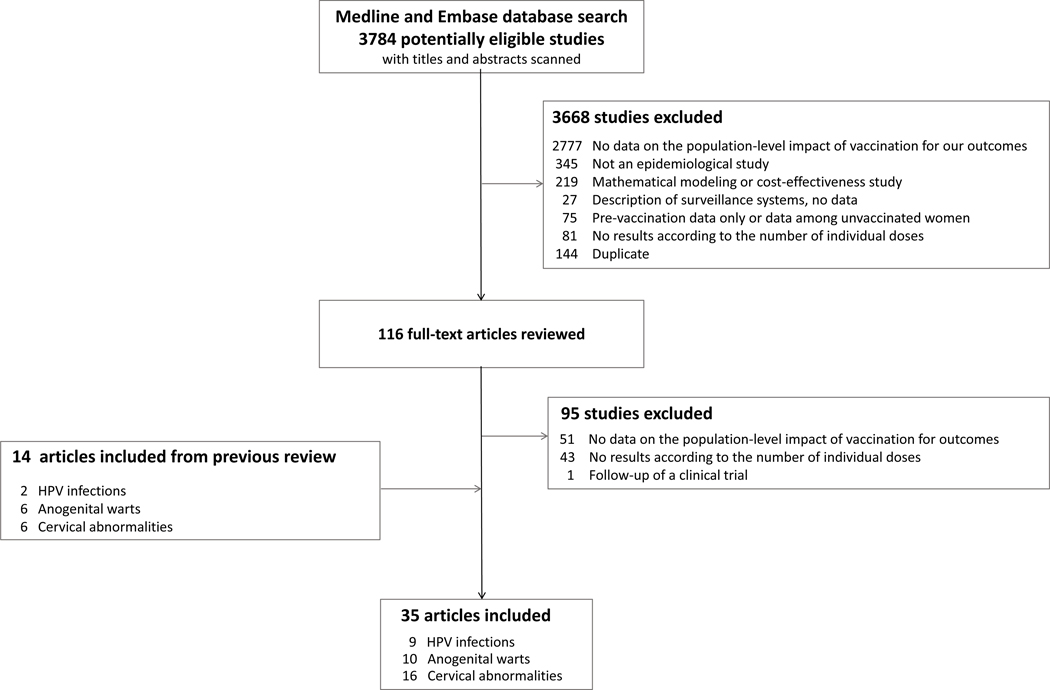
Methods: We searched Medline and Embase databases from January 1, 2007, through September 29, 2021. Data were extracted and summarized in a narrative synthesis. We also conducted quality assessments for bias due to selection, information, and confounding.
Results: Overall, 35 studies were included; all except one were conducted within the context of a recommended three-dose schedule. Evaluations were in countries that used bivalent HPV vaccine (seven), quadrivalent HPV vaccine (27) or both (one). Nine evaluated effectiveness against HPV infection, ten anogenital warts, and 16 cervical abnormalities. All studies were judged to have moderate or serious risk of bias. The biases rated as serious would likely result in lower effectiveness with fewer doses. Investigators attempted to control for or stratify by potentially important variables, such as age at vaccination. Eight studies evaluated impact of buffer periods (lag time) for case counting and 10 evaluated different intervals between doses for two-dose vaccine recipients. Studies that stratified by vaccination age found higher effectiveness with younger age at vaccination, although differences were not all formally tested. Most studies found highest estimates of effectiveness with three doses; significant effectiveness was found among 28/29 studies that evaluated three doses, 19/29 that evaluated two doses, and 18/30 that evaluated one dose. Some studies that adjusted or stratified analyses by age at vaccination found similar effectiveness with three, two and one doses.
Conclusion: Observational studies of HPV vaccine effectiveness have many biases. Studies examining persons vaccinated prior to sexual activity and using methods to reduce sources of bias are needed for valid effectiveness estimates.
Keywords: HPV; HPV vaccine; Human papillomavirus; Vaccine effectiveness.
Published by Elsevier Ltd.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. LM, MD, MJ, JMB, GO, ARK, and MB are members of the Single-Dose HPV vaccine evaluation consortium.
Figures
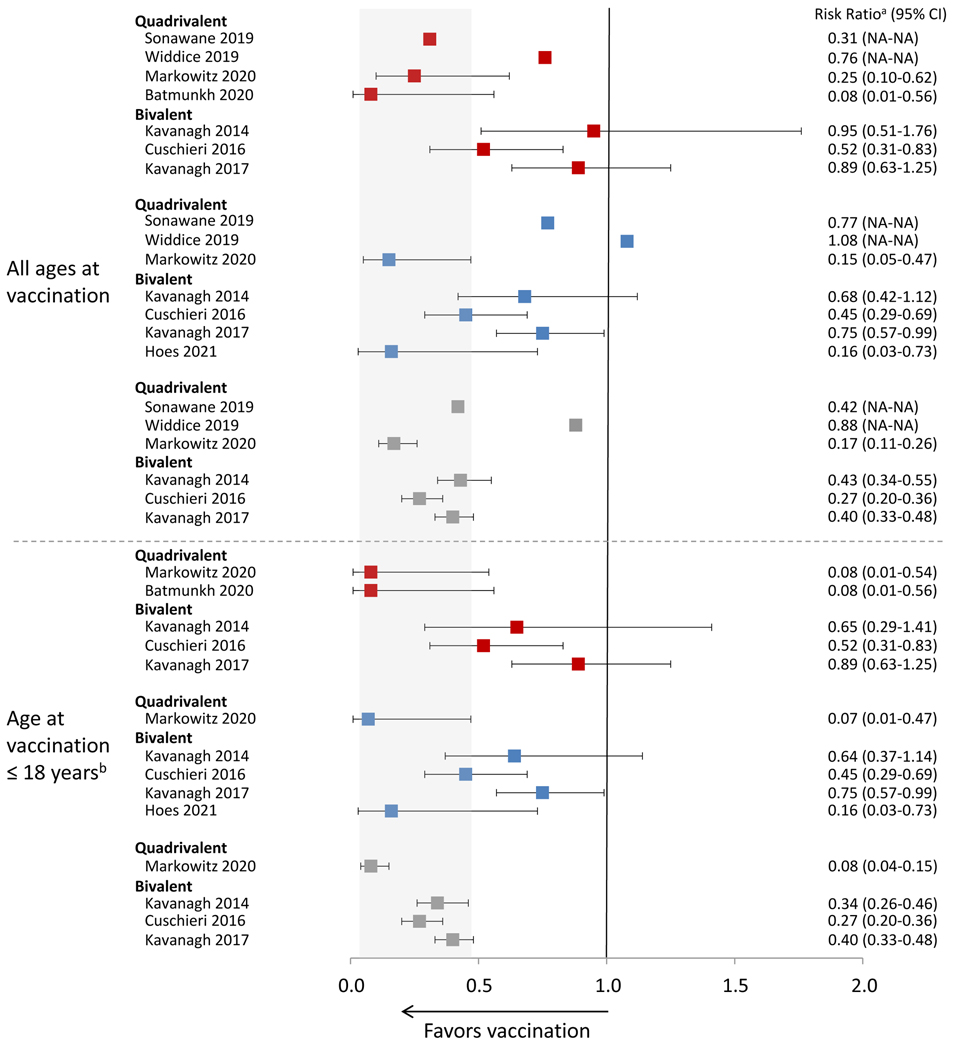
 1 dose vs 0 doses;
1 dose vs 0 doses;  2 doses vs 0 doses;
2 doses vs 0 doses;  3 doses vs 0 doses Data included in this analysis were extracted from original published articles. NA, not available Gray area indicates the range of the CIs from the published studies for effectiveness of 3 doses among girls aged 18 or younger when vaccinated. aRisk ratio includes different measures depending on study, including incidence rate ratio, prevalence ratio, risk ratio, odds ratio or hazard ratio; for Widdice 2019 and Sonawane 2019, risk ratio was estimated from the prevalence of HPV infection among the different dose groups presented in the article, but the authors did not formally assess the effectiveness of 1,2,3 doses compared to 0 dose. bAge at vaccination ≤18 years of age varied by study; for Markowitz 2020, ≤18 years; for Batmunkh 2020, age 11–17 years; for Kavanagh 2014, estimates from an analysis adjusted for birth cohort and there were few individuals vaccinated at age >18 years; for Cushieri 2016, estimates from an analysis adjusted by birth cohort and there were few individuals vaccinated at age >18 years; for Kavanagh 2017 estimates from an analysis adjusted for birth cohort and there were few individuals vaccinated at age >18 years.
3 doses vs 0 doses Data included in this analysis were extracted from original published articles. NA, not available Gray area indicates the range of the CIs from the published studies for effectiveness of 3 doses among girls aged 18 or younger when vaccinated. aRisk ratio includes different measures depending on study, including incidence rate ratio, prevalence ratio, risk ratio, odds ratio or hazard ratio; for Widdice 2019 and Sonawane 2019, risk ratio was estimated from the prevalence of HPV infection among the different dose groups presented in the article, but the authors did not formally assess the effectiveness of 1,2,3 doses compared to 0 dose. bAge at vaccination ≤18 years of age varied by study; for Markowitz 2020, ≤18 years; for Batmunkh 2020, age 11–17 years; for Kavanagh 2014, estimates from an analysis adjusted for birth cohort and there were few individuals vaccinated at age >18 years; for Cushieri 2016, estimates from an analysis adjusted by birth cohort and there were few individuals vaccinated at age >18 years; for Kavanagh 2017 estimates from an analysis adjusted for birth cohort and there were few individuals vaccinated at age >18 years.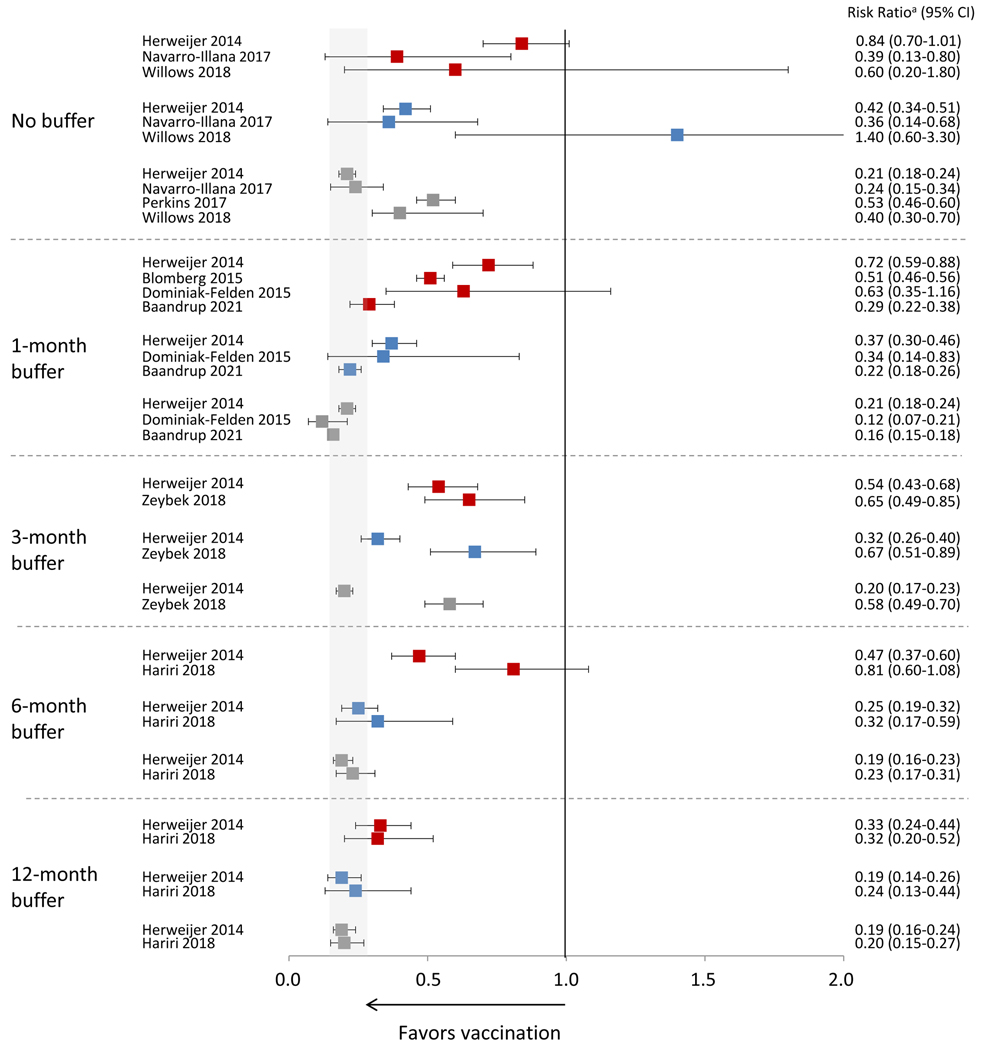
 1 dose vs 0 doses;
1 dose vs 0 doses;  2 doses vs 0 doses;
2 doses vs 0 doses;  3 doses vs 0 doses Data included in this analysis were extracted from original published articles. Gray area indicates the range of the CIs from the published studies for effectiveness of 3 doses using the longest buffer period. Perkins reports using a buffer period but does not report results in the article. a Risk ratio includes different measures depending on study, including incidence rate ratio, prevalence ratio, risk ratio, odds ratio or hazard ratio.
3 doses vs 0 doses Data included in this analysis were extracted from original published articles. Gray area indicates the range of the CIs from the published studies for effectiveness of 3 doses using the longest buffer period. Perkins reports using a buffer period but does not report results in the article. a Risk ratio includes different measures depending on study, including incidence rate ratio, prevalence ratio, risk ratio, odds ratio or hazard ratio.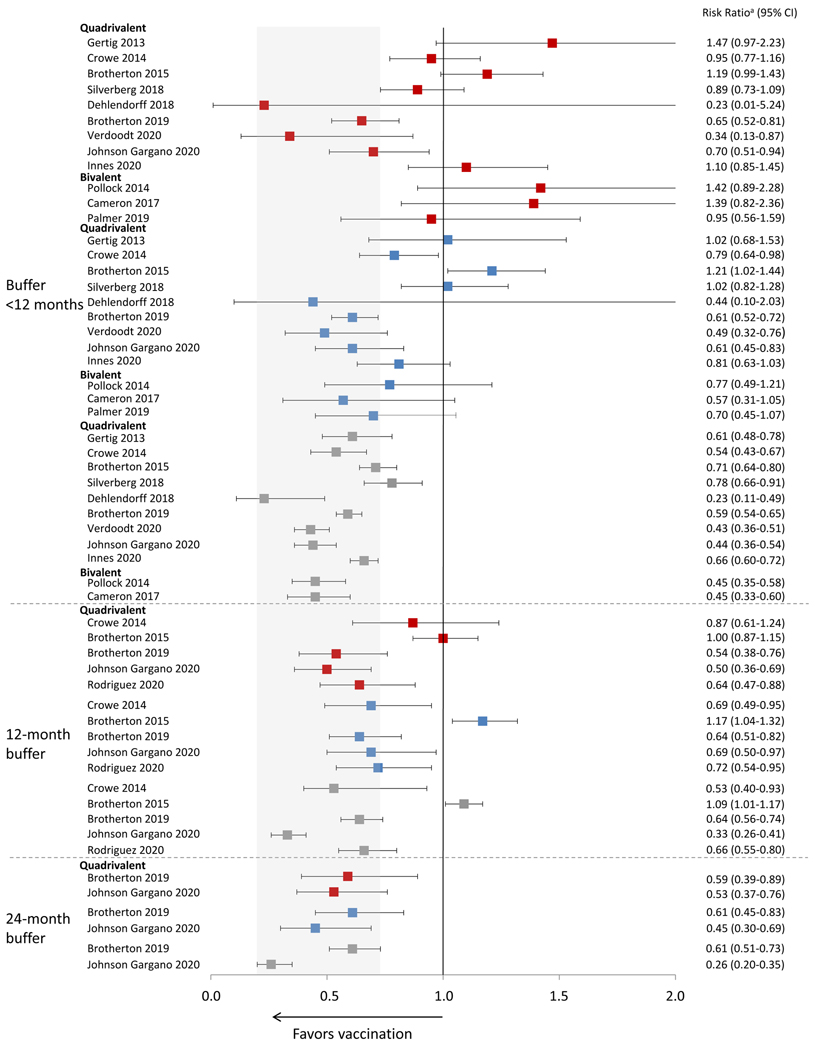
 1 dose vs 0 doses;
1 dose vs 0 doses;  2 doses vs 0 doses;
2 doses vs 0 doses;  3 doses vs 0 doses Data included in this analysis were extracted from original published articles. Gray area indicates the range of the CIs from the published studies for effectiveness of 3 doses using the longest buffer period. CIN2+, cervical intraepithelial neoplasia grade 2, 3, or worse or adenocarcinoma in situ a Risk ratio includes different measures depending on study, including incidence rate ratio, prevalence ratio, risk ratio, odds ratio, or hazard ratio.
3 doses vs 0 doses Data included in this analysis were extracted from original published articles. Gray area indicates the range of the CIs from the published studies for effectiveness of 3 doses using the longest buffer period. CIN2+, cervical intraepithelial neoplasia grade 2, 3, or worse or adenocarcinoma in situ a Risk ratio includes different measures depending on study, including incidence rate ratio, prevalence ratio, risk ratio, odds ratio, or hazard ratio.References
-
- Iversen OE, Miranda MJ, Ulied A, Soerdal T, Lazarus E, Chokephaibulkit K, et al. Immunogenicity of the 9-valent HPV vaccine using 2-dose regimens in girls and boys vs a 3-dose regimen in women. JAMA. 2016;316:2411–21. - PubMed
-
- Dobson SR, McNeil S, Dionne M, Dawar M, Ogilvie G, Krajden M, et al. Immunogenicity of 2 doses of HPV vaccine in younger adolescents vs 3 doses in young women: a randomized clinical trial. JAMA. 2013;309:1793–802. - PubMed
-
- WHO. Human papillomavirus vaccines: WHO position paper, October 2014. Wkly Epidemiol Rec. 2014;89:465–91. - PubMed
-
- Meites E, Kempe A, Markowitz LE. Use of a 2-dose schedule for human papillomavirus vaccination - updated recommendations of the Advisory Committee on Immunization Practices. MMWR Morb Mortal Wkly Rep. 2016;65:1405–8. - PubMed
