

Clinical and imaging features of diabetic striatopathy: report of 6 cases and literature review
- PMID: 35965280
- PMCID: PMC9376124
- DOI: 10.1007/s10072-022-06342-y
Clinical and imaging features of diabetic striatopathy: report of 6 cases and literature review
Abstract
Objective: To explore the clinical manifestations, diagnosis, treatment, and pathogenesis of diabetic striatopathy (DS) to improve the understanding of the disease and avoid misdiagnosis or underdiagnosis.
Methods: The clinical, laboratory, and imaging data of 6 patients (5 Asian females and 1 Asian male) with diabetic striatum were analyzed retrospectively, and the related literature was reviewed.
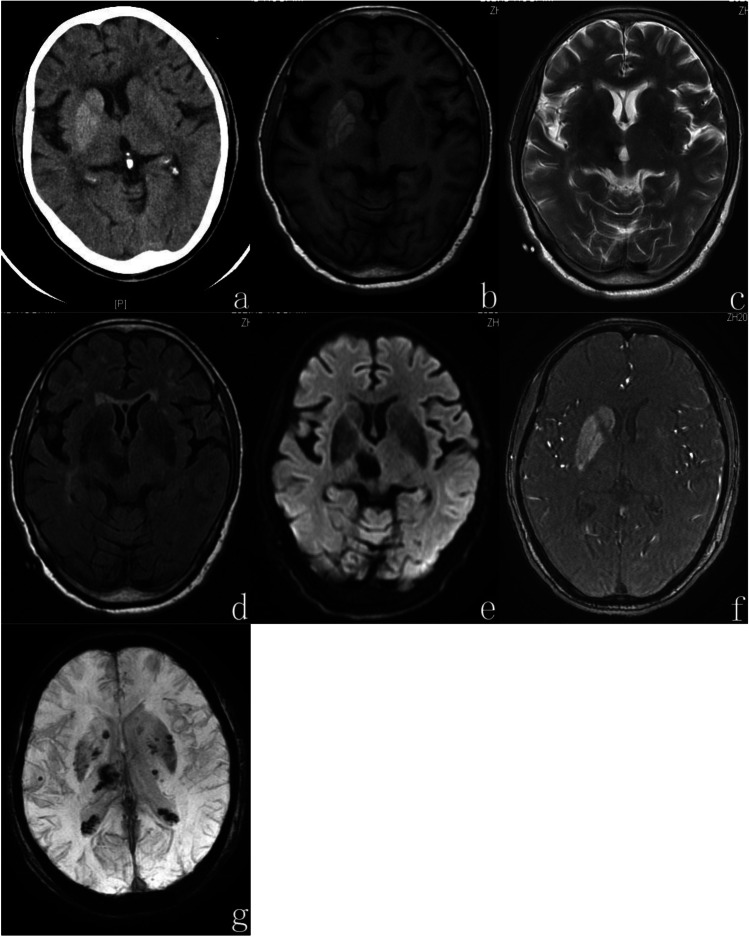
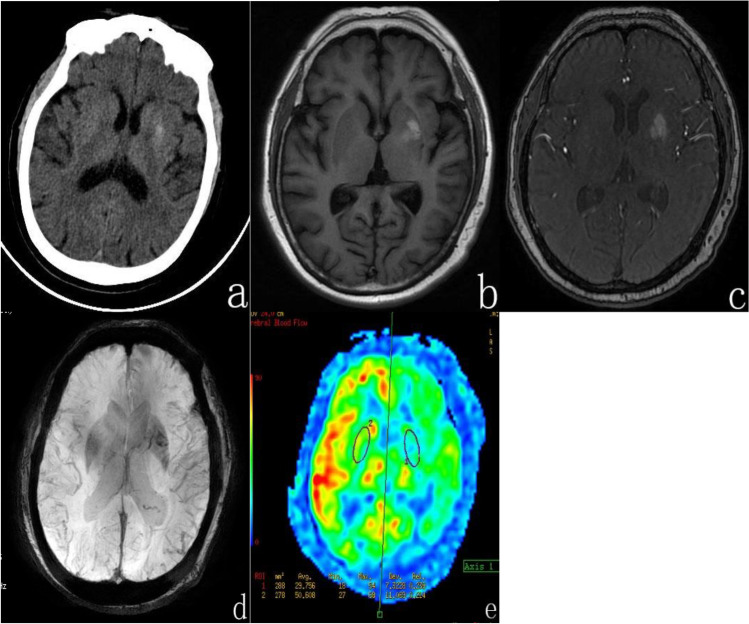
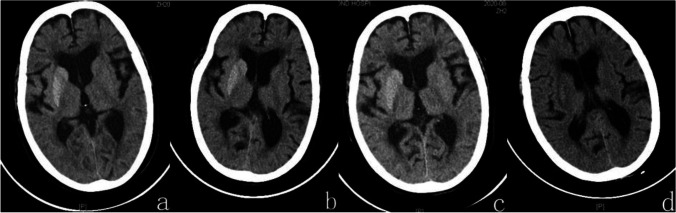
Results: All 6 patients showed hyperglycemia, 5 patients presented with involuntary movement of unilateral limbs, and 1 with unilateral limb numbness. Besides, 5 patients (except case 3) underwent MRI examinations that showed hyperintensity in unilateral caudate and lentiform nucleus on T1-weighted images. And all 6 patients who underwent brain CT examinations showed hyperdensity or isodensity in unilateral caudate and lentiform nucleus. None had a family history of similar abnormal movements. After blood glucose control and symptomatic support treatment, the symptoms of all patients improved to various degrees, and reexaminations showed that the lesions gradually disappeared.
Conclusion: Diabetic striatal disease is a rare complication of diabetes mellitus, the result of a combination of different pathogenesis. It is characterized by hyperglycemia, hemichorea, and contralateral striatal T1WI hyperintensity or CT hyperdensity. Both ketosis and nonketotic hyperglycemic hemichorea have typical imaging manifestations. The prognosis is excellent when this disease is detected early, and the lesions can be gradually absorbed and dissipated with glycemic control.
Keywords: Computed tomography; Diabetic striatopathy; Hemichorea; Hyperglycemia; Magnetic resonance image.
© 2022. Fondazione Società Italiana di Neurologia.
Conflict of interest statement
The authors declare no competing interests.
Figures



Similar articles
-
Diabetic striatopathy: an updated overview of current knowledge and future perspectives.J Endocrinol Invest. 2024 Jan;47(1):1-15. doi: 10.1007/s40618-023-02166-5. Epub 2023 Aug 14. J Endocrinol Invest. 2024. PMID: 37578646 Free PMC article. Review.
-
Neuroimaging of Diabetic Striatopathy: More Questions than Answers.Eur Neurol. 2022;85(5):371-376. doi: 10.1159/000524936. Epub 2022 Jun 17. Eur Neurol. 2022. PMID: 35717942 Review.
-
Nonketotic hyperglycemia hemichorea and hemiballismus: a case report.J Med Case Rep. 2024 Mar 12;18(1):154. doi: 10.1186/s13256-023-04332-y. J Med Case Rep. 2024. PMID: 38468351 Free PMC article.
-
Clinical and neuroimaging characteristics of diabetic striatopathy: a case series report.Front Endocrinol (Lausanne). 2024 Dec 10;15:1429026. doi: 10.3389/fendo.2024.1429026. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 39720255 Free PMC article.
-
Is diabetic striatopathy the culprit of seizures in a patient with ketotic hyperglycemia-induced hemichorea-hemiballismus?BMC Neurol. 2022 Apr 8;22(1):133. doi: 10.1186/s12883-022-02659-5. BMC Neurol. 2022. PMID: 35395738 Free PMC article.
Cited by
-
Diabetic striatopathy in type 1 diabetes mellitus: a rare conundrum.BMJ Case Rep. 2023 Dec 30;16(12):e257448. doi: 10.1136/bcr-2023-257448. BMJ Case Rep. 2023. PMID: 38160036
-
Cognitive decline as the main manifestation of diabetic striatal disease but without involuntary movements: a case report.BMC Neurol. 2023 Nov 30;23(1):425. doi: 10.1186/s12883-023-03452-8. BMC Neurol. 2023. PMID: 38036957 Free PMC article.
-
A Case Report and Literature Review of Nonketotic Hyperglycemic Hemichorea.Cureus. 2024 Mar 13;16(3):e56087. doi: 10.7759/cureus.56087. eCollection 2024 Mar. Cureus. 2024. PMID: 38618383 Free PMC article.
-
A Case of Non-ketotic Hyperglycemic Hemichorea-Hemiballismus in a 54-Year-Old Male Individual With Type 2 Diabetes Mellitus.Cureus. 2025 Jan 22;17(1):e77820. doi: 10.7759/cureus.77820. eCollection 2025 Jan. Cureus. 2025. PMID: 39991375 Free PMC article.
-
Investigation of the factors associated with hemichorea/hemiballismus in post-stroke patients.J Neural Transm (Vienna). 2023 May;130(5):679-685. doi: 10.1007/s00702-023-02628-3. Epub 2023 Apr 3. J Neural Transm (Vienna). 2023. PMID: 37010612
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
