

Relations of Current and Past Cancer with Severe Outcomes among 104,590 Hospitalized COVID-19 Patients: The COVID EHR Cohort at the University of Wisconsin
- PMID: 35965473
- PMCID: PMC9827105
- DOI: 10.1158/1055-9965.EPI-22-0500
Relations of Current and Past Cancer with Severe Outcomes among 104,590 Hospitalized COVID-19 Patients: The COVID EHR Cohort at the University of Wisconsin
Abstract
Background: There is mixed evidence about the relations of current versus past cancer with severe COVID-19 outcomes and how they vary by patient and cancer characteristics.
Methods: Electronic health record data of 104,590 adult hospitalized patients with COVID-19 were obtained from 21 United States health systems from February 2020 through September 2021. In-hospital mortality and ICU admission were predicted from current and past cancer diagnoses. Moderation by patient characteristics, vaccination status, cancer type, and year of the pandemic was examined.
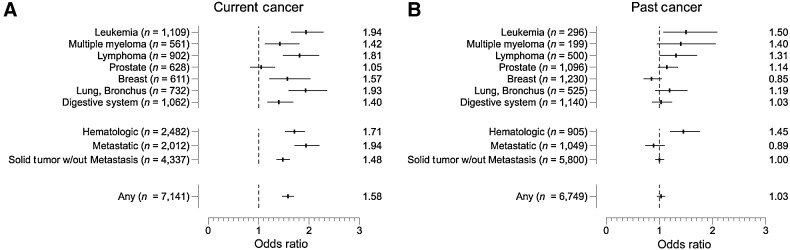
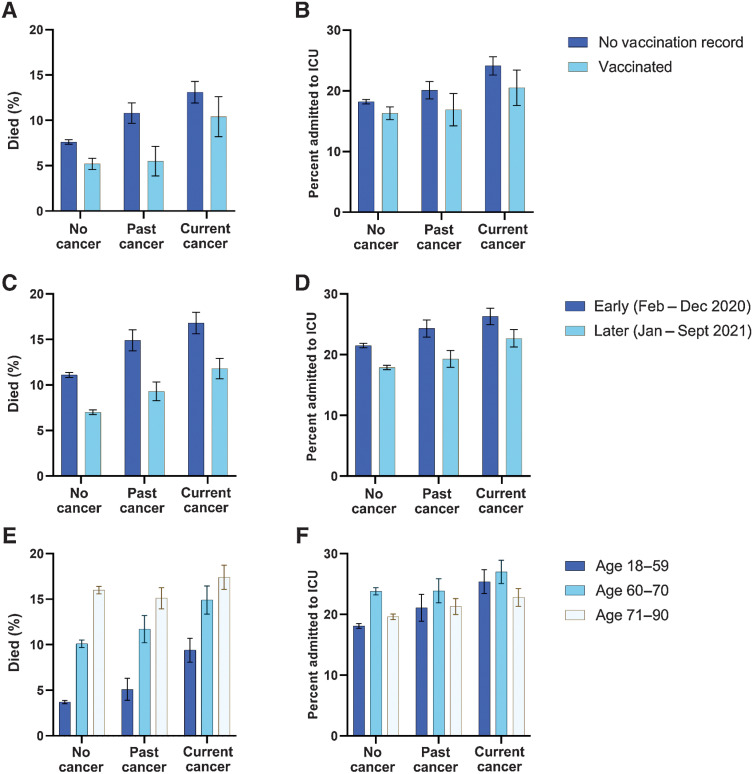
Results: 6.8% of the patients had current (n = 7,141) and 6.5% had past (n = 6,749) cancer diagnoses. Current cancer predicted both severe outcomes but past cancer did not; adjusted odds ratios (aOR) for mortality were 1.58 [95% confidence interval (CI), 1.46-1.70] and 1.04 (95% CI, 0.96-1.13), respectively. Mortality rates decreased over the pandemic but the incremental risk of current cancer persisted, with the increment being larger among younger vs. older patients. Prior COVID-19 vaccination reduced mortality generally and among those with current cancer (aOR, 0.69; 95% CI, 0.53-0.90).
Conclusions: Current cancer, especially among younger patients, posed a substantially increased risk for death and ICU admission among patients with COVID-19; prior COVID-19 vaccination mitigated the risk associated with current cancer. Past history of cancer was not associated with higher risks for severe COVID-19 outcomes for most cancer types.
Impact: This study clarifies the characteristics that modify the risk associated with cancer on severe COVID-19 outcomes across the first 20 months of the COVID-19 pandemic. See related commentary by Egan et al., p. 3.
©2022 The Authors; Published by the American Association for Cancer Research.
Figures
Comment in
-
The Importance of Recency of Cancer Diagnosis in Patients Hospitalized with COVID-19-Glimpses from an EHR-based Study.Cancer Epidemiol Biomarkers Prev. 2023 Jan 9;32(1):3-5. doi: 10.1158/1055-9965.EPI-22-0876. Cancer Epidemiol Biomarkers Prev. 2023. PMID: 36620898
References
-
- American Association for Cancer Research. AACR report on the impact of COVID-19 on cancer research and patient care. Philadelphia, PA: American Association for Cancer Research, 2022[cited 2022 April 27]. Available from: https://www.aacr.org/professionals/research/aacr-covid-19-and-cancer-rep.... - PubMed
