

The efficacy and safety of blunt impingement followed by a sharp recanalization technique in hemodialysis patients with refractory central vein occlusion: a single-center experience
- PMID: 35965835
- PMCID: PMC9372654
- DOI: 10.21037/atm-22-3131
The efficacy and safety of blunt impingement followed by a sharp recanalization technique in hemodialysis patients with refractory central vein occlusion: a single-center experience
Abstract
Background: Central vein occlusion (CVO) is a serious problem in hemodialysis patients. There is an unsatisfactory result for refractory CVO by sharp recanalization alone. This study evaluated the efficacy and safety of blunt impingement followed by sharp recanalization for the treatment of CVO in hemodialysis patients.
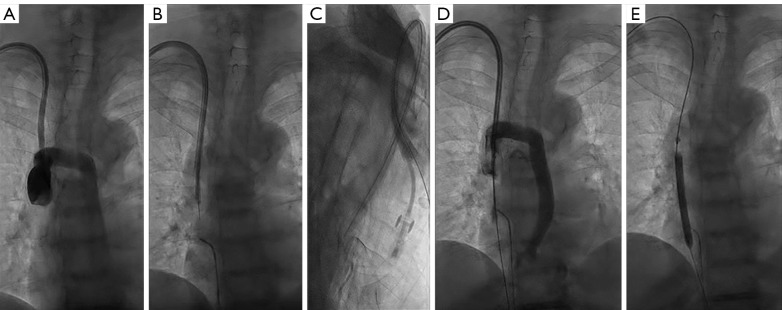
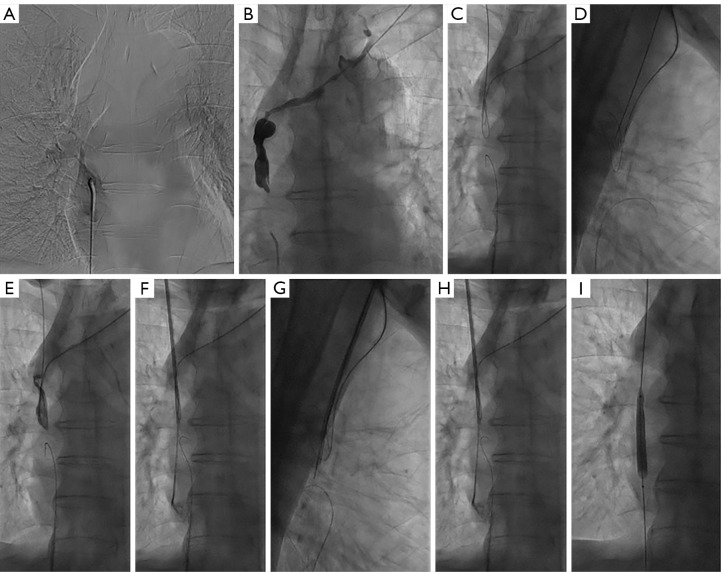
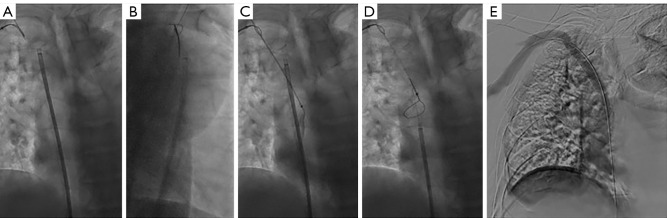
Methods: This study retrospectively examined hemodialysis patients with CVO who failed to recanalize using standard guidewire and catheter techniques in our department. In the first instance, all CVOs were recanalized using blunt impingement techniques, including a 6-Fr long sheath (Cook Incorporated, Bloomington, IN USA) and an 8-Fr sheath of Rosch-Uchida Transjugular Liver Access Set (RUPS-100; Cook Incorporated, Bloomington, IN, USA). If this was not successful, sharp recanalization devices were applied, including the stiff tip of a guidewire (Terumo, Tokyo, Japan), the RUPS-100, and the percutaneous transhepatic cholangial drainage (PTCD) needle (Cook Incorporated, USA). All patients were followed up at least 4 months postoperatively. The technical success rate, arteriovenous access patency rates, and operation-related complications were analyzed.
Results: The procedural success rate was 100.0% (30 of 30). Thirty patients with CVO underwent blunt impingement with a technique success rate of 70.0% (21 of 30), and 9 patients received sharp recanalization after failed blunt impingement, with a technique success rate of 100.0% (9 of 9). The primary patency rates at 6 and 12 months postoperatively were 86.7% and 53.3%, respectively. The primary assisted patency rates were 93.3% and 63.3%, and the secondary patency rates were 93.3% and 70.0% at 6 and 12 months, respectively. One major procedure-related complication was detected, namely, a small injury of the superior vena cava (SVC) wall in a patient receiving recanalization via the stiff end of a guidewire, but this did not require further treatment.
Conclusions: It is potentially effective and safe for interventionalists to use blunt impingement followed by sharp recanalization techniques to treat chronic CVO that is refractory to traversal using traditional catheter and guidewire techniques.
Keywords: Blunt impingement; hemodialysis; refractory central venous occlusion; sharp recanalization.
2022 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://atm.amegroups.com/article/view/10.21037/atm-22-3131/coif). The authors have no conflicts of interest to declare.
Figures



References
LinkOut - more resources
Full Text Sources