

Anesthetic and analgesic techniques and perioperative inflammation may affect the timing of recurrence after complete resection for non-small-cell lung cancer
- PMID: 35965864
- PMCID: PMC9373037
- DOI: 10.3389/fsurg.2022.886241
Anesthetic and analgesic techniques and perioperative inflammation may affect the timing of recurrence after complete resection for non-small-cell lung cancer
Abstract
Introduction: It has been widely recognized that both surgery and anesthesia may increase the risk of cancer recurrence by inducing an inflammatory response and immunosuppression in various cancer operations. The present study explored using hazard curves how anesthetic and analgesic techniques regarding the host inflammation status affect the risk of recurrence over time in patients with non-small-cell lung cancer (NSCLC).
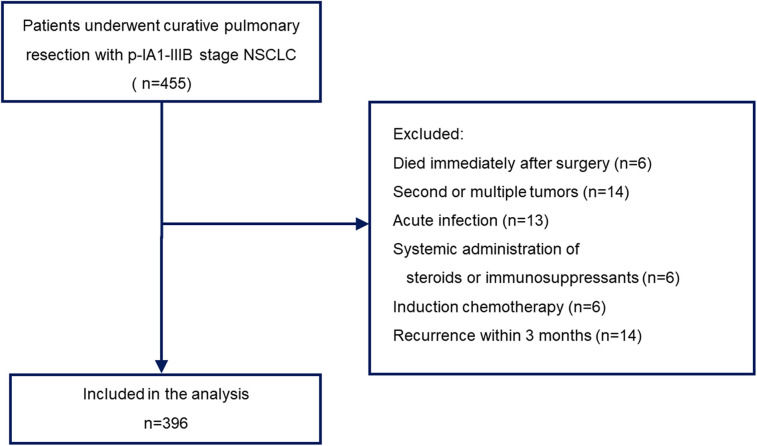
Material and methods: Clinicopathological data from patients who underwent complete pulmonary resection with pathological I-IIIB stage NSCLC from 2010 to 2020 were collected. The inflammation-based scores, including the C-reactive protein-to-albumin ratio (CAR), systemic immune-inflammation index (SII), Glasgow prognostic score (GPS), and modified GPS (mGPS), were calculated before surgery, and hazard curves indicating the changes in hazards over time were evaluated.
Results: A total of 396 patients were eligible for the analysis. The median follow-up was 42.3 months. In total, 118 patients (29.8%) experienced recurrence, and 66.9% of those occurred within 24 months after surgery. According to the multivariate Cox regression analysis, volatile anesthesia (VA) (hazard ratio [HR], 1.69; 95% confidence interval [CI], 1.05-2.71), and elevated CAR (HR, 1.88; 95% CI, 1.18-2.99) were associated with a worse recurrence-free survival. The resulting hazard curve revealed that a delayed peak of recurrence was present in patients with a low CAR in the VA group and in those with intravenous flurbiprofen axetil administration in the propofol-based total intravenous anesthesia group (30 and 24 months after surgery, respectively).
Discussion: Choosing anesthetic and analgesic techniques while taking inflammation-based scores into account may be useful for reducing the risk of and/or delaying recurrence in patients undergoing resection for NSCLC.
Keywords: anesthetic technique; hazard curve; inflammation-based score; multimodal analgesia; non-small-cell lung cancer; recurrence.
© 2022 Watanabe, Masuda and Noma.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
-
- Schack A, Fransgaard T, Klein MF, Gogenur I. Perioperative use of nonsteroidal anti-inflammatory drugs decreases the risk of recurrence of cancer after colorectal resection: a cohort study based on prospective data. Ann Surg Oncol. (2019) 26(12):3826–37. 10.1245/s10434-019-07600-8 PMID: - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials