

Effect of intraoperative dexmedetomidine on hepatic ischemia-reperfusion injury in pediatric living-related liver transplantation: A propensity score matching analysis
- PMID: 35965870
- PMCID: PMC9365069
- DOI: 10.3389/fsurg.2022.939223
Effect of intraoperative dexmedetomidine on hepatic ischemia-reperfusion injury in pediatric living-related liver transplantation: A propensity score matching analysis
Abstract
Background: Hepatic ischemia-reperfusion injury (HIRI) is largely unavoidable during liver transplantation (LT). Dexmedetomidine (DEX), an α2-adrenergic agonist, exerts a variety of organ-protective effects in pediatric populations. However, evidence remains relatively limited about its hepatoprotective effects in pediatric living-related LT.
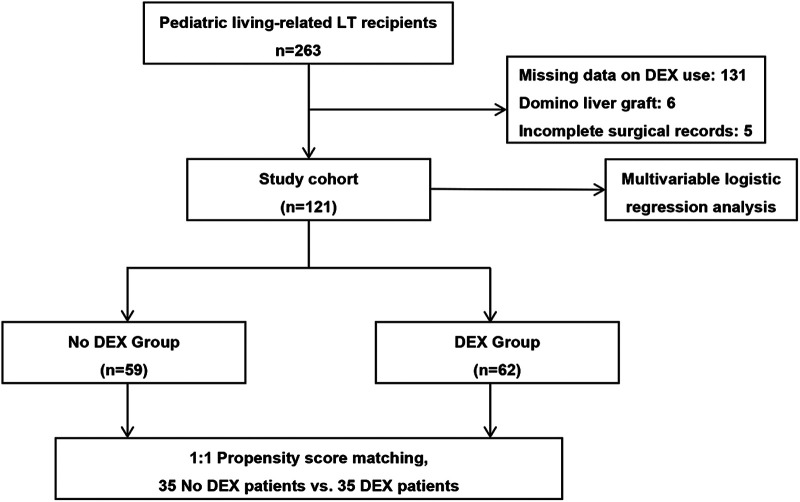
Methods: A total of 121 pediatric patients undergoing living-related LT from June 2015 to December 2018 in our hospital were enrolled. They were classified into DEX or non-DEX groups according to whether an infusion of DEX was initiated from incision to the end of surgery. Primary outcomes were postoperative liver graft function and the severity of HIRI. Multivariate logistic regression and propensity score matching (PSM) analyses were performed to identify any association.
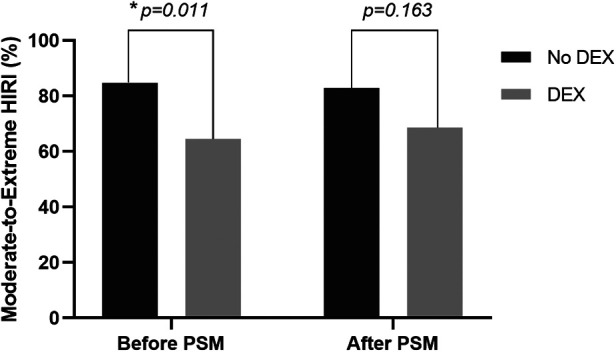
Results: A 1:1 matching yielded 35 well-balanced pairs. Before matching, no significant difference was found in baseline characteristics between groups except for warm ischemia time, which was longer in the non-DEX group (44 [38-50] vs. 40 [37-44] min, p = 0.017). After matching, the postoperative peak lactic dehydrogenase levels decreased significantly in the DEX group than in the non-DEX group (622 [516-909] vs. 970 [648-1,490] IU/L, p = 0.002). Although there was no statistical significance, a tendency toward a decrease in moderate-to-extreme HIRI rate was noted in the DEX group compared to the non-DEX group (68.6% vs. 82.9%, p = 0.163). Patients in the DEX group also received a significantly larger dosage of epinephrine as postreperfusion syndrome (PRS) treatment (0.28 [0.17-0.32] vs. 0.17 [0.06-0.30] µg/kg, p = 0.010). However, there were no significant differences between groups in PRS and acute kidney injury incidences, mechanical ventilation duration, intensive care unit, and hospital lengths of stay. Multivariate analysis revealed a larger graft-to-recipient weight ratio (odds ratio [OR] 2.657, 95% confidence interval [CI], 1.132-6.239, p = 0.025) and intraoperative DEX administration (OR 0.333, 95% CI, 0.130-0.851, p = 0.022) to be independent predictors of moderate-to-extreme HIRI.
Conclusion: This study demonstrated that intraoperative DEX could potentially decrease the risk of HIRI but was associated with a significant increase in epinephrine requirement for PRS in pediatric living-related LT. Further studies, including randomized controlled studies, are warranted to provide more robust evidence.
Keywords: dexmedetomidine; ischemia-reperfusion injury; liver transplantation; pediatrics; postreperfusion syndrome.
© 2022 Zhang, Cui, Yang, Xue and Zhu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Effect of dexmedetomidine on liver transplantation: a meta-analysis.Front Pharmacol. 2023 May 22;14:1188011. doi: 10.3389/fphar.2023.1188011. eCollection 2023. Front Pharmacol. 2023. PMID: 37292152 Free PMC article.
-
Dexmedetomidine Cannot Attenuate Liver Injury and Improve Outcomes Following Laparoscopic Living Donor Hepatectomy: A Randomised Controlled Trial.Drug Des Devel Ther. 2025 May 22;19:4263-4274. doi: 10.2147/DDDT.S524343. eCollection 2025. Drug Des Devel Ther. 2025. PMID: 40420947 Free PMC article. Clinical Trial.
-
Intraoperative Low-Dose Dexmedetomidine Administration Associated with Reduced Hepatic Ischemia-Reperfusion Injury in Pediatric Deceased Liver Transplantation: A Retrospective Cohort Study.Ann Transplant. 2021 Oct 15;26:e933354. doi: 10.12659/AOT.933354. Ann Transplant. 2021. PMID: 34650026 Free PMC article.
-
Impact of Paired Remote Ischemic Preconditioning on Postreperfusion Syndrome in Living-Donor Liver Transplantation: A Propensity-Score Matching Analysis.Medicina (Kaunas). 2024 Nov 7;60(11):1830. doi: 10.3390/medicina60111830. Medicina (Kaunas). 2024. PMID: 39597016 Free PMC article.
-
Perioperative dexmedetomidine reduces delirium in elderly patients after non-cardiac surgery: a systematic review and meta-analysis of randomized-controlled trials.Can J Anaesth. 2019 Dec;66(12):1489-1500. doi: 10.1007/s12630-019-01440-6. Epub 2019 Jul 1. Can J Anaesth. 2019. PMID: 31264195 English.
Cited by
-
The Effect of Dexmedetomidine and Levobupivacaine in an Experimental Ischemia Reperfusion Model.In Vivo. 2024 Nov-Dec;38(6):2696-2704. doi: 10.21873/invivo.13747. In Vivo. 2024. PMID: 39477431 Free PMC article.
-
Effect of dexmedetomidine on liver transplantation: a meta-analysis.Front Pharmacol. 2023 May 22;14:1188011. doi: 10.3389/fphar.2023.1188011. eCollection 2023. Front Pharmacol. 2023. PMID: 37292152 Free PMC article.
-
Protective Effects of Trimetazidine and Dexmedetomidine on Liver Injury in a Mesenteric Artery Ischemia-Reperfusion Rat Model via Endoplasmic Reticulum Stress.Biomedicines. 2024 Oct 10;12(10):2299. doi: 10.3390/biomedicines12102299. Biomedicines. 2024. PMID: 39457612 Free PMC article.
-
Dexmedetomidine Cannot Attenuate Liver Injury and Improve Outcomes Following Laparoscopic Living Donor Hepatectomy: A Randomised Controlled Trial.Drug Des Devel Ther. 2025 May 22;19:4263-4274. doi: 10.2147/DDDT.S524343. eCollection 2025. Drug Des Devel Ther. 2025. PMID: 40420947 Free PMC article. Clinical Trial.
-
Current status and perspective on molecular targets and therapeutic intervention strategy in hepatic ischemia-reperfusion injury.Clin Mol Hepatol. 2024 Oct;30(4):585-619. doi: 10.3350/cmh.2024.0222. Epub 2024 Jul 1. Clin Mol Hepatol. 2024. PMID: 38946464 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Miscellaneous