

Brain-Lung Crosstalk: Management of Concomitant Severe Acute Brain Injury and Acute Respiratory Distress Syndrome
- PMID: 35965956
- PMCID: PMC9363869
- DOI: 10.1007/s11940-022-00726-3
Brain-Lung Crosstalk: Management of Concomitant Severe Acute Brain Injury and Acute Respiratory Distress Syndrome
Abstract
Purpose of review: To summarize pathophysiology, key conflicts, and therapeutic approaches in managing concomitant severe acute brain injury (SABI) and acute respiratory distress syndrome (ARDS).
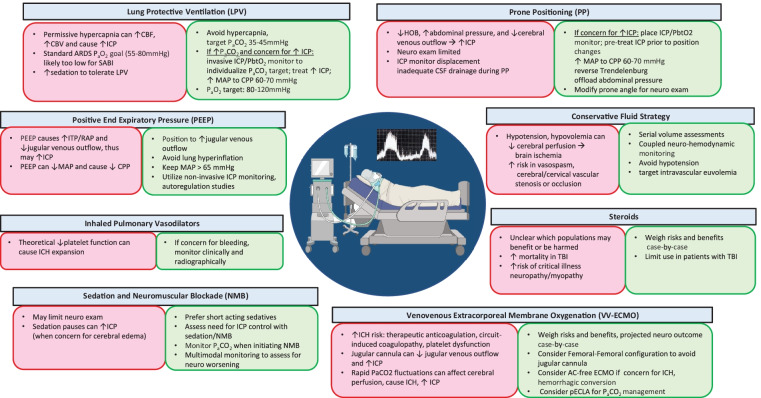
Recent findings: ARDS is common in SABI and independently associated with worse outcomes in all SABI subtypes. Most landmark ARDS trials excluded patients with SABI, and evidence to guide decisions is limited in this population. Potential areas of conflict in the management of patients with both SABI and ARDS are (1) risk of intracranial pressure (ICP) elevation with high levels of positive end-expiratory pressure (PEEP), permissive hypercapnia due to lung protective ventilation (LPV), or prone ventilation; (2) balancing a conservative fluid management strategy with ensuring adequate cerebral perfusion, particularly in patients with symptomatic vasospasm or impaired cerebrovascular blood flow; and (3) uncertainty about the benefit and harm of corticosteroids in this population, with a mortality benefit in ARDS, increased mortality shown in TBI, and conflicting data in other SABI subtypes. Also, the widely adapted partial pressure of oxygen (PaO2) target of > 55 mmHg for ARDS may exacerbate secondary brain injury, and recent guidelines recommend higher goals of 80-120 mmHg in SABI. Distinct pathophysiology and trajectories among different SABI subtypes need to be considered.
Summary: The management of SABI with ARDS is highly complex, and conventional ARDS management strategies may result in increased ICP and decreased cerebral perfusion. A crucial aspect of concurrent management is to recognize the risk of secondary brain injury in the individual patient, monitor with vigilance, and adjust management during critical time windows. The care of these patients requires meticulous attention to oxygenation and ventilation, hemodynamics, temperature management, and the neurological exam. LPV and prone ventilation should be utilized, and supplemented with invasive ICP monitoring if there is concern for cerebral edema and increased ICP. PEEP titration should be deliberate, involving measures of hemodynamic, pulmonary, and brain physiology. Serial volume status assessments should be performed in SABI and ARDS, and fluid management should be individualized based on measures of brain perfusion, the neurological exam, and cardiopulmonary status. More research is needed to define risks and benefits in corticosteroids in this population.
Keywords: Acute ischemic stroke; Acute lung injury; Acute respiratory distress syndrome; Cardiac arrest; Hypoxemic ischemic encephalopathy; Intracranial hemorrhage; Severe acute brain injury; Subarachnoid hemorrhage; Traumatic brain injury.
© The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature 2022.
Conflict of interest statement
Conflict of InterestWe report no conflicts of interests, and none of the authors has received direct funding for this study. Abhijit Lele receives ongoing salary support from LifeCenter Northwest. Vasisht Srinivasan receives grant support from the Centers for Disease Control and Prevention via the Influenza and Other Viruses in the Acute Ill (IVY) network. Nicholas Johnson receives funding from the National Institutes of Health, from the Centers for Disease Control and Prevention, the Department of Defense, and the UW Royalty Research Fund for unrelated work. The remaining authors report no financial disclosures.
Figures


References
References and Recommended Reading
Papers of particular interest, published recently, have been highlighted as: • Of importance
-
- Holland MC, Mackersie RC, Morabito D, et al. The development of acute lung injury is associated with worse neurologic outcome in patients with severe traumatic brain injury. J Trauma. 2003;55(1):106–111. doi: 10.1097/01.TA.0000071620.27375.BE. - DOI - PubMed
-
- Bratton SL, Davis RL. Acute lung injury in isolated traumatic brain injury. Neurosurgery. 1997;40(4):707–712; discussion 712. 10.1097/00006123-199704000-00009. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
