

ACTH-independent Cushing's syndrome due to ectopic endocrinologically functional adrenal tissue caused by a GNAS heterozygous mutation: a rare case of McCune-Albright syndrome accompanied by central amenorrhea and hypothyroidism: a case report and literature review
- PMID: 35966069
- PMCID: PMC9373900
- DOI: 10.3389/fendo.2022.934748
ACTH-independent Cushing's syndrome due to ectopic endocrinologically functional adrenal tissue caused by a GNAS heterozygous mutation: a rare case of McCune-Albright syndrome accompanied by central amenorrhea and hypothyroidism: a case report and literature review
Abstract
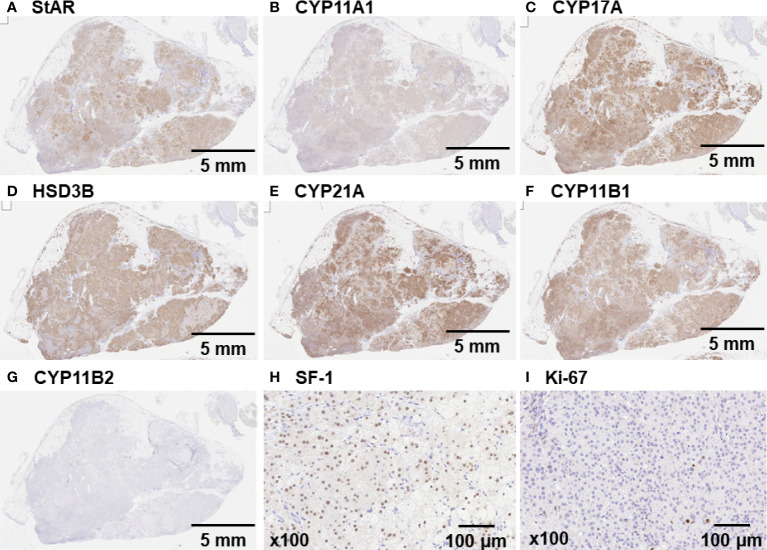
In a small number of cases, the development of ectopic residual adrenal lesions during embryogenesis causing Cushing's syndrome due to the production of excess cortisol has been reported. A 29-year-old woman was admitted to our hospital for fatigue and recent amenorrhea. Her plasma ACTH was <1.5 pg/mL, and her serum cortisol was 21.4 pg/mL after the 8 mg dexamethasone suppression test, revealing the presence of ACTH-independent Cushing's syndrome; however, her bilateral adrenal glands were atrophied. Abdominal CT revealed a 40-mm round tumor on the right renal hilum and remarkably accumulated 131I-labelled adosterol. CT and bone scintigraphy showed that 99mTc-methylene diphosphonate had accumulated in her dissymmetric skull at the right-frontoparietal region. The tumor on the right renal hilum was laparoscopically removed. Her cortisol levels rapidly decreased to below the normal range, and glucocorticoids were administered to rescue adrenal insufficiency. The resected tumor was yellowish in appearance and 4.5×3.0×2.8 cm in size. Immunohistochemical staining for SF-1, P450scc, CYP17A, CYP21A, and CYP11B1 indicated that this tumor produced cortisol. Exome sequencing analysis revealed that the GNAS heterozygous mutation (c.601C>T, p. Arg201Cys; accession number, NM_000516.5) was found in approximately 20% of the adrenal tumor sample. A mutation of GNAS, encoding the Gsα subunit that mediates GPCR signaling, causes the constitutive activation of adenylyl cyclase, resulting in hypersecretion of hormones regulated by the GPCR. GNAS mutation is one of the major genetic causes of cortisol-producing adrenal tumors independent of ACTH secretion. Considering the combination of GNAS mutation with one of the typical clinical triad characteristics, fibrous dysplasia of bone, we diagnosed this patient with McCune-Albright syndrome accompanied by ACTH-independent Cushing's syndrome caused by an ectopic residual adrenal tumor due to GNAS mutation. This case highlights that GNAS involves a previously unknown pathological mechanism in which inhibition of the natural elimination of remnant tissue leads to ectopic endocrine hypersecretion.
Keywords: Cushing’s syndrome; GNAS mutation; McCune–Albright syndrome; ectopic adrenal tumor; fibrous dysplasia.
Copyright © 2022 Takedani, Yamamoto, Tanaka, Ishihara, Taketani and Kanasaki.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
The mystery of transient pregnancy-induced cushing's syndrome: a case report and literature review highlighting GNAS somatic mutations and LHCGR overexpression.Endocrine. 2024 Feb;83(2):473-482. doi: 10.1007/s12020-023-03549-7. Epub 2023 Oct 12. Endocrine. 2024. PMID: 37828397 Review.
-
A case of autonomous cortisol secretion in a patient with subclinical Cushing's syndrome, GNAS mutation, and paradoxical cortisol response to dexamethasone.BMC Endocr Disord. 2019 Jan 22;19(1):13. doi: 10.1186/s12902-019-0345-8. BMC Endocr Disord. 2019. PMID: 30670014 Free PMC article.
-
A Novel GNAS Mutation Causing Isolated Infantile Cushing's Syndrome.Horm Res Paediatr. 2019;92(3):196-202. doi: 10.1159/000501169. Epub 2019 Jul 30. Horm Res Paediatr. 2019. PMID: 31362300
-
McCune Albright syndrome and bilateral adrenal hyperplasia: the GNAS mutation may only be present in adrenal tissue.Hormones (Athens). 2015 Jul-Sep;14(3):447-50. doi: 10.14310/horm.2002.1578. Hormones (Athens). 2015. PMID: 26188235 Free PMC article.
-
Association of hypertension and hypokalemia with Cushing's syndrome caused by ectopic ACTH secretion: a series of 58 cases.Ann N Y Acad Sci. 2002 Sep;970:134-44. doi: 10.1111/j.1749-6632.2002.tb04419.x. Ann N Y Acad Sci. 2002. PMID: 12381548 Review.
Cited by
-
The mystery of transient pregnancy-induced cushing's syndrome: a case report and literature review highlighting GNAS somatic mutations and LHCGR overexpression.Endocrine. 2024 Feb;83(2):473-482. doi: 10.1007/s12020-023-03549-7. Epub 2023 Oct 12. Endocrine. 2024. PMID: 37828397 Review.
References
-
- Abdel-Latif ME, Bajuk B, Ward M, Oei JL, Badawi N, NSW and ACT Neonatal Intensive Care Units Audit Group . Neurodevelopmental outcomes of extremely premature infants conceived after assisted conception: a population based cohort study. Arch Dis Child Fetal Neonatal Ed (2013) 98:F205–11. doi: 10.1136/archdischild-2012-302040 - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical