

The effect of various types and doses of statins on C-reactive protein levels in patients with dyslipidemia or coronary heart disease: A systematic review and network meta-analysis
- PMID: 35966518
- PMCID: PMC9363636
- DOI: 10.3389/fcvm.2022.936817
The effect of various types and doses of statins on C-reactive protein levels in patients with dyslipidemia or coronary heart disease: A systematic review and network meta-analysis
Abstract
Objective: The objective of this study was to measure the efficacy of various types and dosages of statins on C-reactive protein (CRP) levels in patients with dyslipidemia or coronary heart disease.
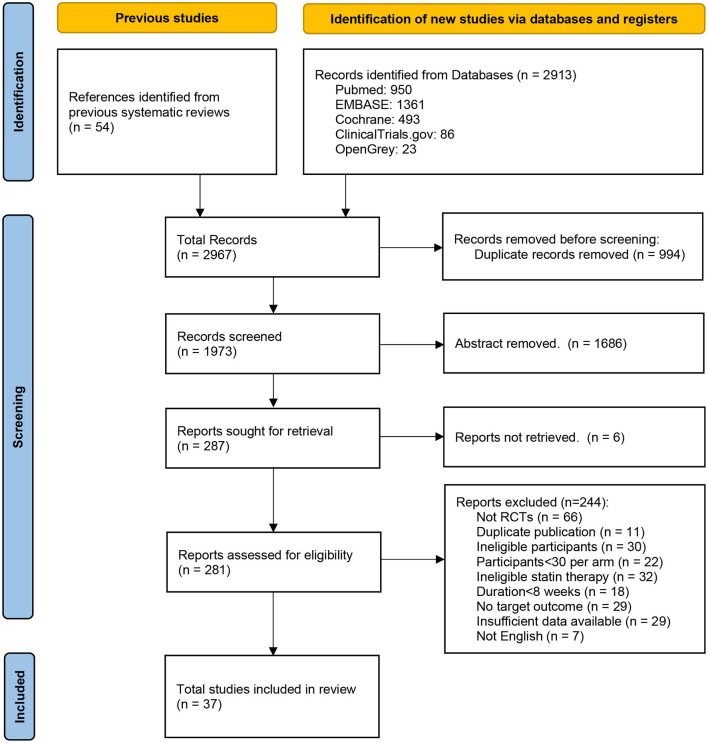
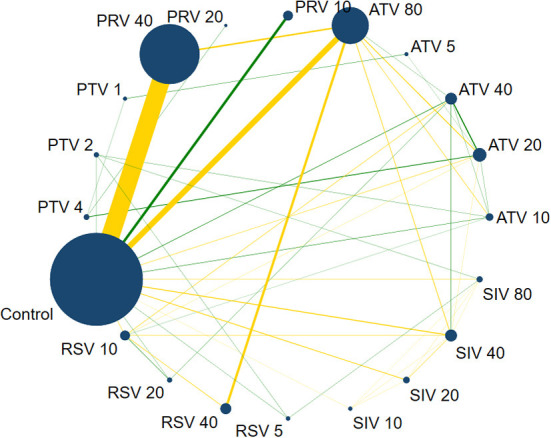
Methods: Randomized controlled trials were searched from PubMed, Embase, Cochrane Library, OpenGray, and ClinicalTrials.gov. We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines for data extraction and synthesis. The pairwise meta-analysis compared statins and controls using a random-effects model, and a network meta-analysis compared the types and dosages of statins using the Bayesian random-effects model. The PROSPERO registration number is CRD42021242067.
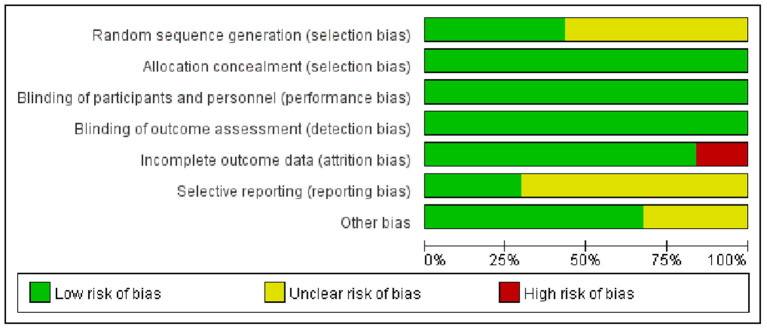
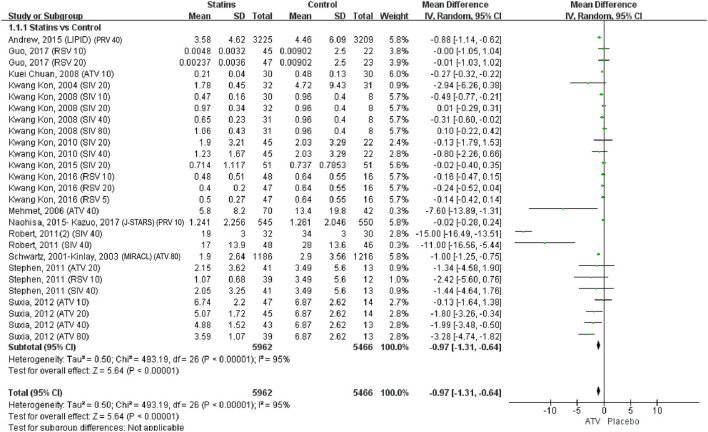
Results: The study included 37 randomized controlled trials with 17,410 participants and 20 interventions. According to the pairwise meta-analysis, statins significantly decreased CRP levels compared to controls (weighted mean difference [WMD] = -0.97, 95% confidence interval [CI] [-1.31, -0.64], P < 0.0001). In the network meta-analysis, simvastatin 40 mg/day appeared to be the best strategy for lowering CRP (Rank P = 0.18, WMD = -4.07, 95% CI = [-6.52, -1.77]). The same was true for the high-sensitivity CRP, non-acute coronary syndrome (ACS), <12 months duration, and clear measurement subgroups. In the CRP subgroup (rank P = 0.79, WMD = -1.23, 95% CI = [-2.48, -0.08]) and ≥12-month duration subgroup (Rank P = 0.40, WMD = -2.13, 95% CI = [-4.24, -0.13]), atorvastatin 80 mg/day was most likely to be the best. There were no significant differences in the dyslipidemia and ACS subgroups (P > 0.05). Node-splitting analysis showed no significant inconsistency (P > 0.05), except for the coronary heart disease subgroup.
Conclusion: Statins reduced serum CRP levels in patients with dyslipidemia or coronary heart disease. Simvastatin 40 mg/day might be the most effective therapy, and atorvastatin 80 mg/day showed the best long-term effect. This study provides a reference for choosing statin therapy based on LDL-C and CRP levels.
Keywords: C-reactive protein; coronary heart disease; dyslipidemia; network meta-analysis; statin.
Copyright © 2022 Zhang, Wang, Tian, Wang, Jia, Lai, Wang, Zhang, Song, Ju and Xu.
Conflict of interest statement
All authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Jellinger PS, Handelsman Y, Rosenblit PD, Bloomgarden ZT, Fonseca VA, Garber AJ, et al. . American Association of Clinical Endocrinologists and American College of Endocrinology Guidelines for management of dyslipidemia and prevention of cardiovascular disease. Endocr Pract. (2017) 23:479–97. 10.4158/EP171764.GL - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous