

Transcatheter Aortic Valve Implantation for Severe Bicuspid Aortic Stenosis - 2 Years Follow up Experience From India
- PMID: 35966565
- PMCID: PMC9369256
- DOI: 10.3389/fcvm.2022.817705
Transcatheter Aortic Valve Implantation for Severe Bicuspid Aortic Stenosis - 2 Years Follow up Experience From India
Abstract
Background: Transcatheter aortic valve implantation (TAVI) is challenging in bicuspid aortic valve (BAV) anatomy. The patients are young, morphological phenotypes are many, calcium burden is high and there are technical challenges for best outcomes. Observational studies and registries are available with favorable data and experiences from around the world sharing methodologies and algorithms for sizing and implantation. We, therefore, analysed our data of procedural and in-hospital outcomes of TAVI in Bicuspid Aortic Valve cases performed at two high volume centres in India and their follow up for two years.
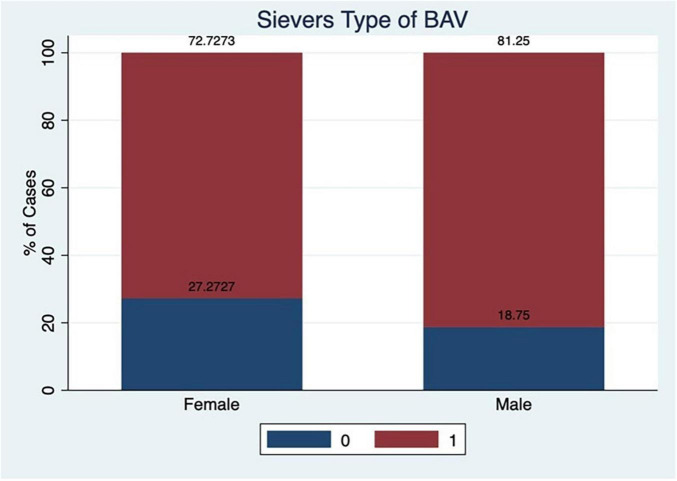
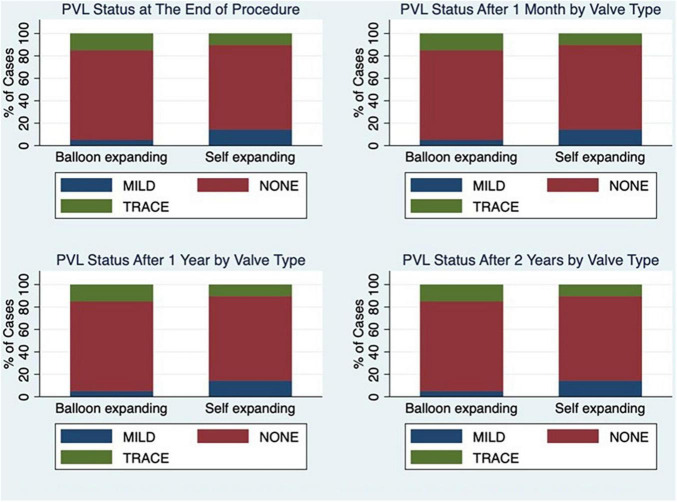
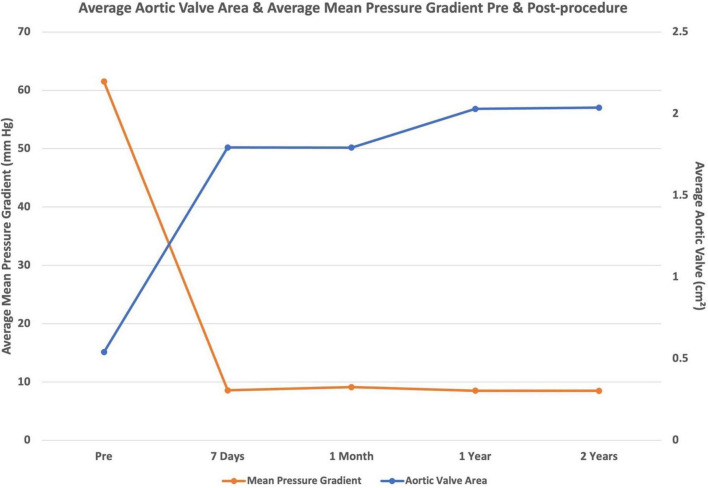
Methods and results: The data were collated and analysed from two centres (Fortis Escorts Heart Institute, New Delhi and Apollo Hospitals, Chennai) in India for patients who underwent TAVI in a BAV anatomy. It included a total of 70 cases from 2 centres. All symptomatic severe AS patients more than and equal to 65 years having bicuspid anatomy were included in the study irrespective of their STS score. Patients under 65 years of age were advised TAVI only if they were at high risk for open heart surgery. These patients were followed for a period of 2 years and the data were analysed. Pre TAVI imaging tools utilised were 2D echo, transthoracic echocardiography (TTE), trans oesophageal echocardiography (TEE), and ECG gated multi slice CT (MSCT) scan imaging. MSCT was utilised for confirmation of the anatomy and classifying the morphological type of valve, measuring, and evaluating all anatomic determinants of aortic root complex for planning the procedure and choice of the valve and its size. Sizing in balloon expanding valve (BEV) and self-expanding valve sizing (SEV) were based primarily on annulus area and perimeter, respectively. The SEV used in our study were the Core Valve and Evolut R (Medtronic, United States) and the BEVs included Sapien3 (Edwards Lifesciences, United States) and Myval (Meril Lifesciences, India). The BAV cohort constituted 24.4% of the total 287 TAVI cases, followed up for 2 years. The mean age of these patients was 72 years. The incidence of male patients was 68.57% and female patients was 31.4%. The Sievers type 1 included 78.5%, type 0 were 21.4% of the cases and there was no case of type 2 in the study. The procedural success was to the tune of 98%. Patients with normal left ventricular ejection fraction (LVEF) improved their symptoms class after TAVI and remained so at 2 years follow up. The poor LVEF subset of patients did not have heart failure admissions and also had improvement in their symptom status. The peak-to-peak aortic valve gradient decreased to 0 mmHg at the end of the procedure in most of the cases. The mean pressure gradient (PG) across the new valve ranged between 0 and 15 mmHg and the aortic valve area (AVA) was close to 2 cm2. These numbers were consistent at 2 years follow up. Significant paravalvular leak (PVL) 24.28% was seen immediately after deployment of the valve in heavily calcified anatomy but it reduced to mild or trivial PVL after post-dilation and one patient needed a second valve to treat PVL. No patient had more than mild PVL with either type of valve at the end of the procedure. Permanent pacemaker implantation (PPI) was required in 11.4% of the patients within 24 h to 7 days of the procedure. No one needed a PPI in the 2 year follow up. Coronary occlusion did not happen to any patient. No patient had a disabling stroke. Non-disabling stroke was seen in 10% of cases and mostly in the first week or 30 days of the procedure and the incidence was more with BEV (14%) as compared to SEV (8%). There was one case of valve embolisation after 24 h of the procedure, which needed a surgical valve replacement. There was no case of annular injury or injury to other parts of the aortic root complex. Two cases had access vessel (femoral artery) thrombosis at end of the procedure and a third patient had proglide related residual stenosis. Two cases had acute kidney injury and needed dialysis. There was no major bleeding complication in any patient. Peri procedural mortality occurred in two patients. Valve thrombosis was seen in one patient after 3 months, which was treated with oral anticoagulation. Valve degeneration and failure or infective endocarditis were not seen in any patient.
Conclusion: The patients with BAV stenosis who underwent TAVI in this study had good procedural success rates and clinical outcomes. The haemodynamics achieved with both SEV and BEV were good at 2 years. The rates of PVL, PPI, and stroke are similar to that of many other studies and registries. PPI rate and non-disabling stroke incidence appear to be higher similar to many studies done. There was no case of coronary occlusion in the study. Meticulous CT analysis of the aortic root complex, selection of appropriate type and size of the valve, and best implantation practices along with cerebral protection will probably be the key to safer and more successful TAVI in this population.
Keywords: Indian population; TAVI – transcatheter aortic valve implantation; aortic stenosis; bicuspid aortic stenosis; bicuspid aortic valve.
Copyright © 2022 Kumar, Sengottuvelu, Singh, Rastogi and Seth.
Conflict of interest statement
AS was Proctor for TAVI and received consulting fee from Meril Lifesciences and Medtronic. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Leon MB, Smith CR, Mack MJ, Makkar RR, Svensson LG, Kodali SK, et al. Transcatheter or surgical aortic-valve replacement in intermediate-risk patients. N Engl J Med. (2016) 374:1609–20. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials