

Cryoballoon ablation for atrial fibrillation: Effects on neuromodulation
- PMID: 35966567
- PMCID: PMC9366392
- DOI: 10.3389/fcvm.2022.958316
Cryoballoon ablation for atrial fibrillation: Effects on neuromodulation
Abstract
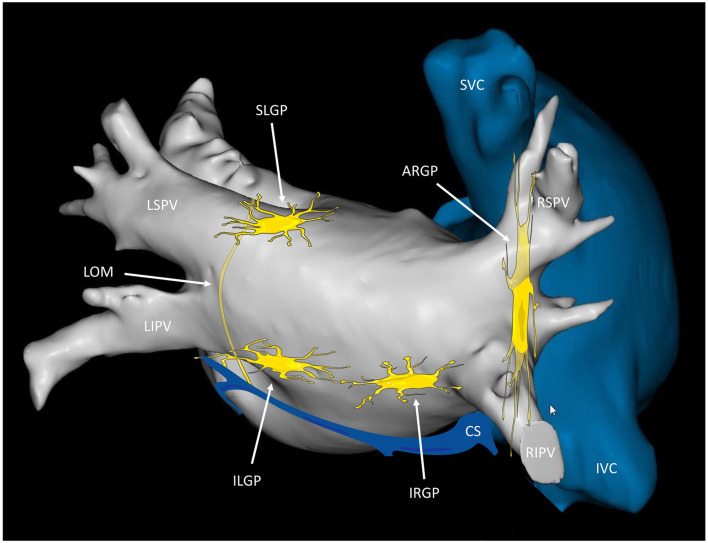
Pulmonary vein isolation (PVI) represents the mainstay of atrial fibrillation (AF) ablation, and PVI with cryoballoon catheter (CB) ablation (CB-A) has proven to be as effective and safe as radiofrequency ablation (RF-A). Although AF is initiated by triggers arising from the pulmonary veins (PV) and non-PV foci, the intrinsic cardiac nervous system (ICNS) plays a significant role in the induction and maintenance of AF. The ICNS is an epicardial neural system composed of ganglionated plexi (GPs) and a complex network of interconnecting neurons. In the left atrium, the major GPs are located in proximity to the PV-left atrial junction. Vagal reactions have been described as markers of autonomic modulation during PVI with both RF-A and CB-A. The occurrence of neuromodulation during PVI with CB-A may be explained by both the anatomical relationship between the GPs and the PVs and the characteristics of the CB. Due to the CB/PV size mismatch, the CB creates a wide ablation area that extends from the PV ostium toward the antrum, possibly including the GPs. Although targeted GPs ablation, as a supplemental strategy to PVI, has been associated with a better AF outcome in patients undergoing RF-A, the additional clinical benefit of neuromodulation during PVI with CB-A remains a matter of debate. In this review, we provide an overview of the anatomy of the ICNS, the relationship between the ICNS and AF pathophysiology, and the current evidence on the clinical relevance of neuromodulation during PVI with CB-A.
Keywords: atrial fibrillation; autonomic denervation; cardiac autonomic nervous system; cryoballoon ablation; ganglionated plexi; neuromodulation.
Copyright © 2022 Del Monte, Pannone, Bisignani, Osório, Iacopino, Chierchia and de Asmundis.
Conflict of interest statement
Author AB is consultant for Biotronik. Author GBC received compensation for teaching purposes and proctoring from Medtronic, Abbott, Biotronik, Boston Scientific, and Acutus Medical. Author CdA receives research grants on behalf of the center from Biotronik, Medtronic, Abbott, LivaNova, Boston Scientific, AtriCure, Philips, Acutus Medical, and received compensation for teaching purposes and proctoring from Medtronic, Abbott, Biotronik, LivaNova, Boston Scientific, AtriCure, Acutus Medical, and Daiichi Sankyo. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Hindricks G, Potpara T, Dagres N, Bax JJ, Boriani G, Dan GA, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. (2021) 42:373–498. 10.1093/eurheartj/ehab648 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials