

Selective endothelial removal: A case series of a phase I/II surgical trial with long-term follow up
- PMID: 35966874
- PMCID: PMC9372295
- DOI: 10.3389/fmed.2022.901187
Selective endothelial removal: A case series of a phase I/II surgical trial with long-term follow up
Abstract
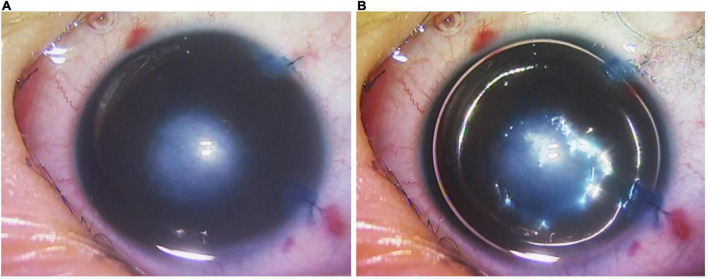
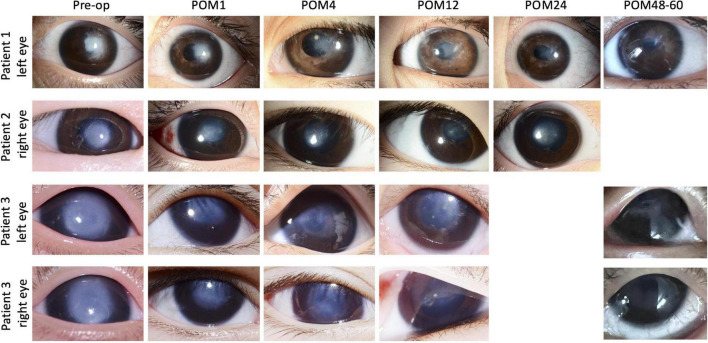
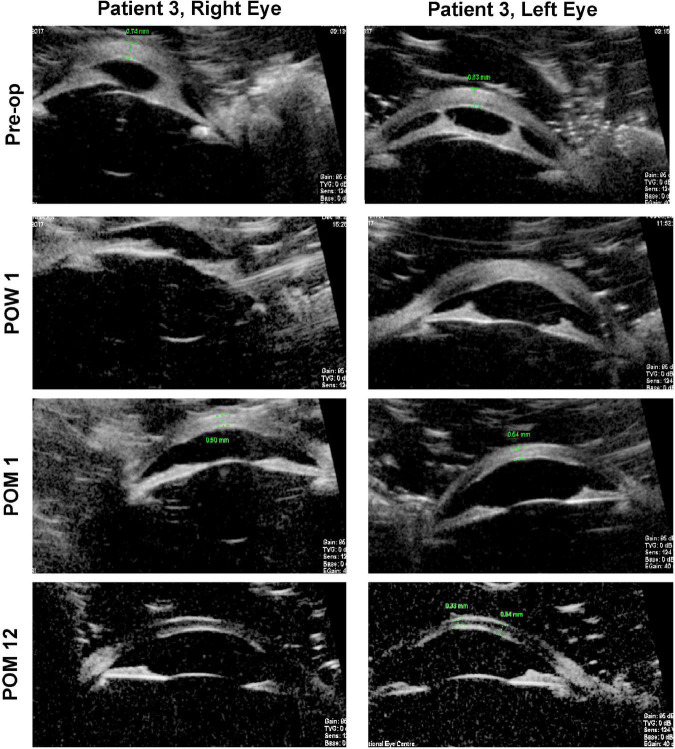
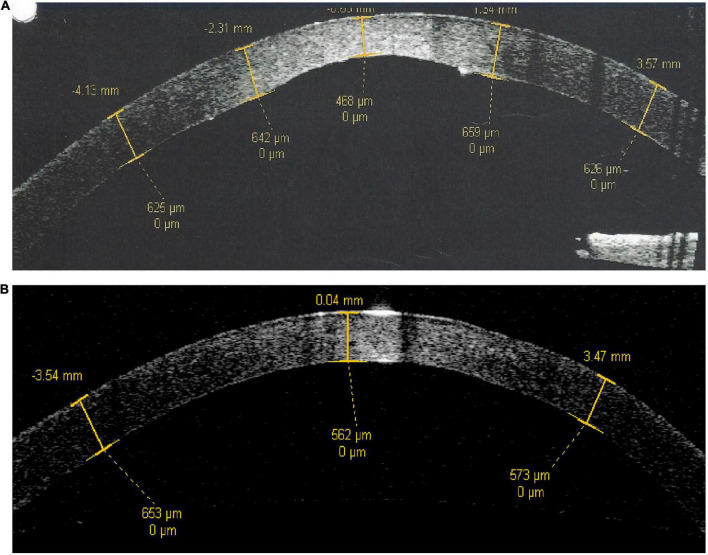
Peters anomaly is a congenital condition which results in a central corneal opacity from birth. Selective Endothelial Removal (SER) is a novel surgical technique and a form of regenerative therapy, which encourages clearance of the central corneal opacity by the patient's own corneal endothelial cells, and it may potentially be beneficial for the treatment of Peters anomaly. We have performed a phase I/II surgical trial, evaluating the safety of SER in four eyes (three patients) with Peters Anomaly. These patients underwent SER at between 9 and 39 months of age, each demonstrating clearance of central corneal opacities and improvements in vision post-operatively. No complications occurred in any of these eyes, at a minimal post-operative follow-up duration of 48 months. We conclude that SER for Peters anomaly is a safe surgical procedure. While encouraging efficacy outcomes have been observed, these findings should be further evaluated in a larger scale Phase II/III surgical trial.
Keywords: Peters anomaly; cornea; endothelium; keratoplasty; regenerative medicine.
Copyright © 2022 Liu, Soh, Kocaba and Mehta.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources