

Mesentery in Transanal TME
- PMID: 35966978
- PMCID: PMC9365469
- DOI: 10.1055/s-0042-1748887
Mesentery in Transanal TME
Abstract
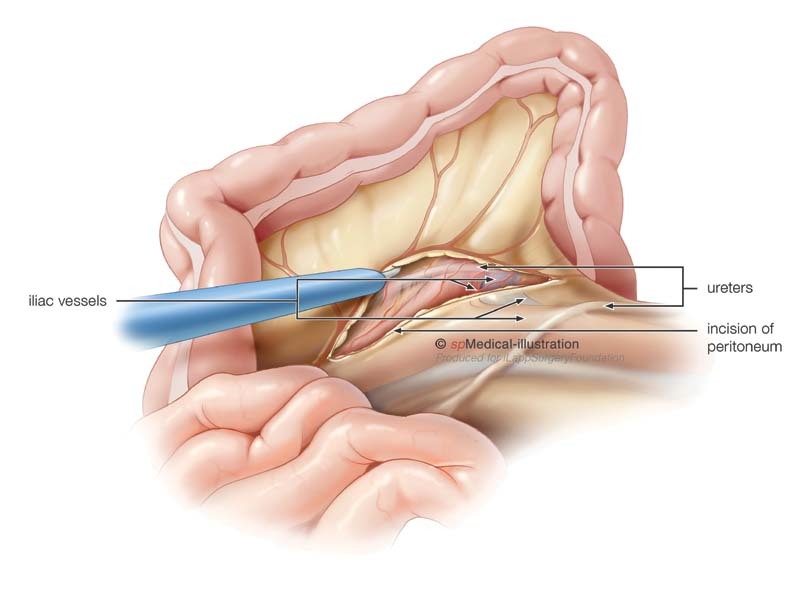
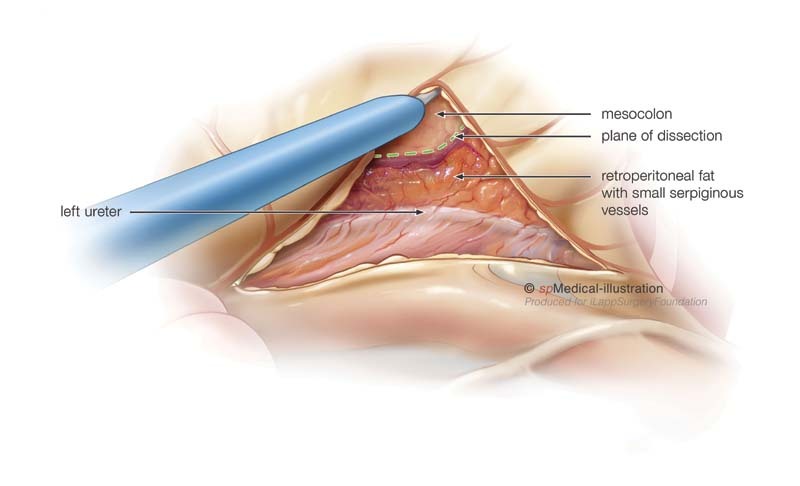
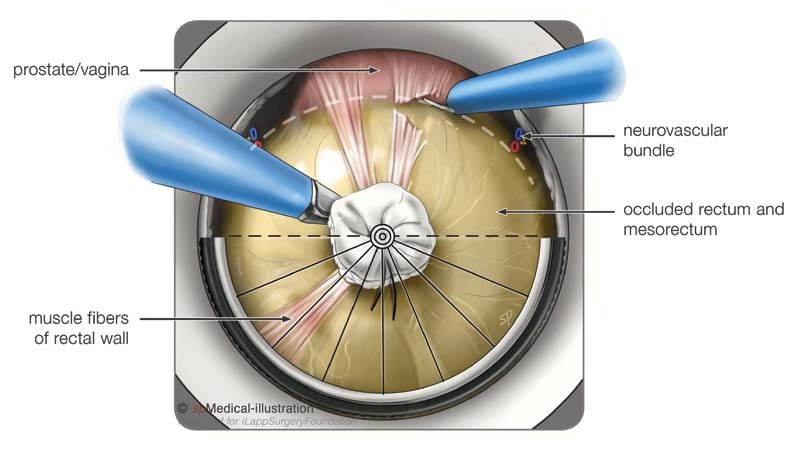
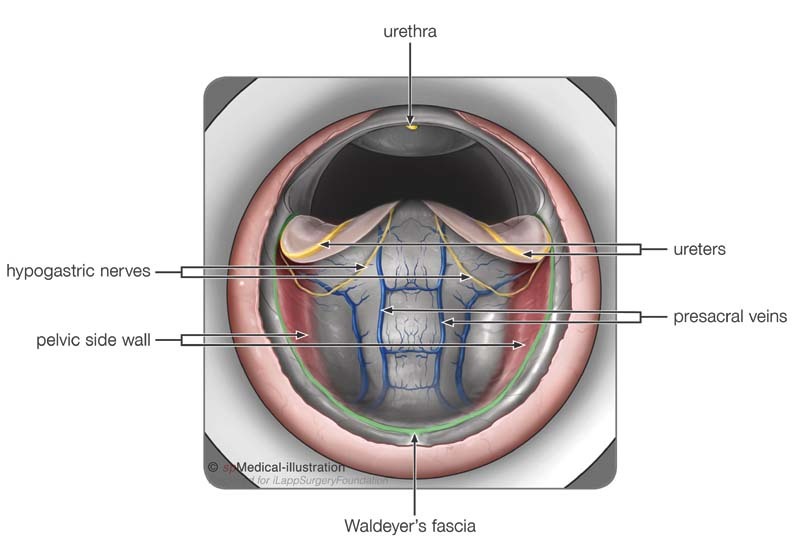
Oncological adequacy in rectal cancer surgery mandates not only a clear distal and circumferential resection margin but also resection of the entire ontogenetic mesorectal package. Incomplete removal of the mesentery is one of the commonest causes of local recurrences. The completeness of the resection is not only determined by tumor and patient related factors but also by the patient-tailored treatment selected by the multidisciplinary team. This is performed in the context of the technical ability and experience of the surgeon to ensure an optimal total mesorectal excision (TME). In TME, popularized by Professor Heald in the early 1980s as a sharp dissection through the avascular embryologic plane, the midline pedicle of tumor and mesorectum is separated from the surrounding, mostly paired structures of the retroperitoneum. Although TME significantly improved the oncological and functional results of rectal cancer surgery, the difficulty of the procedure is still mainly dependent on and determined by the dissection of the most distal part of the rectum and mesorectum. To overcome some of the limitations of working in the narrowest part of the pelvis, robotic and transanal surgery have been shown to improve the access and quality of resection in minimally invasive techniques. Whatever technique is chosen to perform a TME, embryologically derived planes and anatomical points of reference should be identified to guide the surgery. Standardization of the chosen technique, widespread education, and training of surgeons, as well as caseloads per surgeon, are important factors to optimize outcomes. In this article, we discuss the introduction of transanal TME, with emphasis on the mesentery, relevant anatomy, standard procedural steps, and importance of a training pathway.
Keywords: mesentery; rectal cancer; total mesorectal excision; transanal total mesorectal excision.
Thieme. All rights reserved.
Conflict of interest statement
Conflict of Interest None declared.
Figures
Similar articles
-
Total Mesorectal Excision Technique-Past, Present, and Future.Clin Colon Rectal Surg. 2020 May;33(3):134-143. doi: 10.1055/s-0039-3402776. Epub 2020 Apr 28. Clin Colon Rectal Surg. 2020. PMID: 32351336 Free PMC article. Review.
-
Transanal total mesorectal excision (taTME) for rectal cancer: a training pathway.Surg Endosc. 2016 Sep;30(9):4130-5. doi: 10.1007/s00464-015-4680-1. Epub 2015 Dec 10. Surg Endosc. 2016. PMID: 26659246
-
Long-term outcomes by a transanal approach to total mesorectal excision for rectal cancer.Surg Endosc. 2017 Dec;31(12):5248-5257. doi: 10.1007/s00464-017-5597-7. Epub 2017 Jun 22. Surg Endosc. 2017. PMID: 28643051
-
Robotic Transanal Total Mesorectal Excision (RTaTME): State of the Art.J Pers Med. 2021 Jun 21;11(6):584. doi: 10.3390/jpm11060584. J Pers Med. 2021. PMID: 34205596 Free PMC article. Review.
-
[Transanal total mesorectal excision-a critical appraisal].Chirurg. 2019 Jun;90(6):478-486. doi: 10.1007/s00104-019-0945-x. Chirurg. 2019. PMID: 30911795 Review. German.
References
-
- Höckel M. Cancer permeates locally within ontogenetic compartments: clinical evidence and implications for cancer surgery. Future Oncol. 2012;8(01):29–36. - PubMed
-
- Höckel M, Horn L C, Manthey N. Resection of the embryologically defined uterovaginal (Müllerian) compartment and pelvic control in patients with cervical cancer: a prospective analysis. Lancet Oncol. 2009;10(07):683–692. - PubMed
-
- Rodríguez-Luna M R, Guarneros-Zárate J E, Tueme-Izaguirre J.Total mesorectal excision, an erroneous anatomical term for the gold standard in rectal cancer treatment Int J Surg 201523(Pt A):97–100. - PubMed
-
- Dattani M, Santiago I, Mahadevan V, Heald R J.The mesorectum and mesocolon - Making sense of words Int J Surg 201636( Pt A):390–391. - PubMed
