

The Independent Effects of Procurement Biopsy Findings on 10-Year Outcomes of Extended Criteria Donor Kidney Transplants
- PMID: 35967103
- PMCID: PMC9366372
- DOI: 10.1016/j.ekir.2022.05.027
The Independent Effects of Procurement Biopsy Findings on 10-Year Outcomes of Extended Criteria Donor Kidney Transplants
Abstract
Introduction: The role of procurement biopsies in deceased donor kidney evaluation is debated in light of uncertainty about the influence of biopsy findings on recipient outcomes. The literature is filled with conflicting and ambiguous findings typically derived from small studies focused on short-term outcomes or reliant on biopsies prepared by methods impractical in the time-sensitive context of organ procurement.
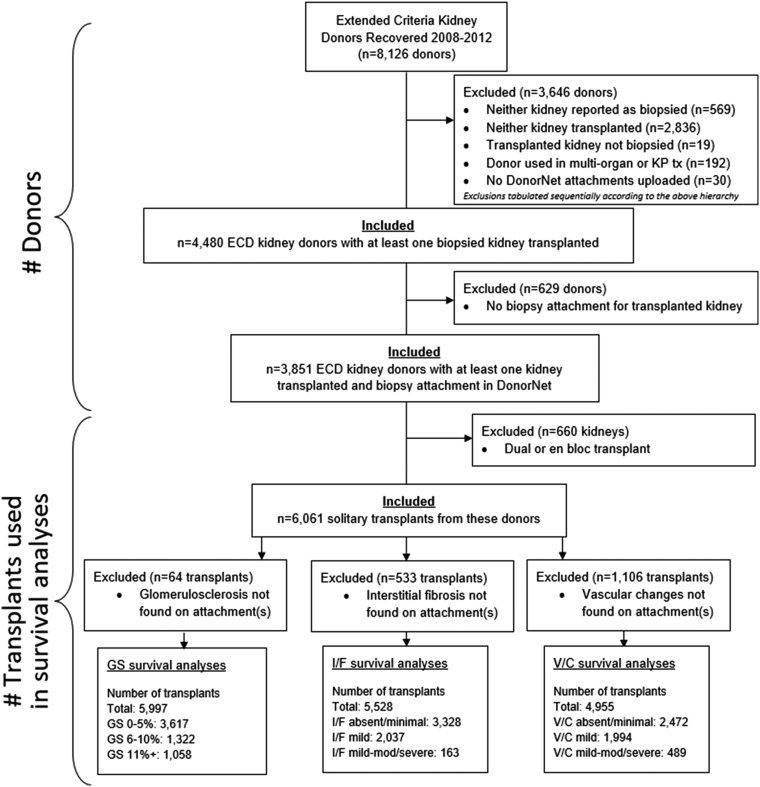
Methods: After manual data entry of DonorNet attachments from 4480 extended criteria donors (ECDs) recovered in the United States from 2008 to 2012, we applied causal inference methods in a Cox regression framework to estimate independent effects of glomerulosclerosis (GS), interstitial fibrosis, and vascular changes on long-term kidney graft survival. Kidney discard rates from 2018 to 2019 were evaluated to characterize contemporary kidney utilization patterns.
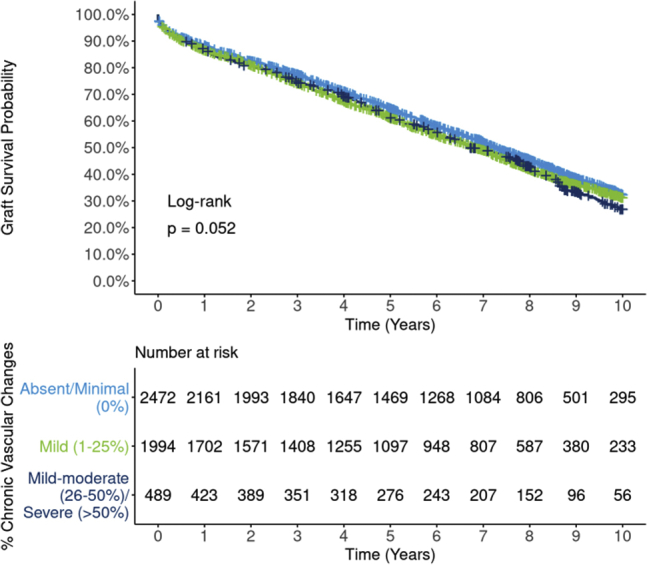
Results: Effects of interstitial fibrosis and vascular changes were largely attenuated after adjusting for potentially confounding donor and recipient variables, although conclusions are less certain for severe levels due to smaller sample sizes. By contrast, significant effects of GS (>10% vs. 0%-5%) persisted even after adjustment (all-cause, hazard ratio [HR] 1.18; 95% CI 1.06, 1.28; death-censored, HR 1.28; 95% CI 1.08, 1.46) but plateaued beyond 10%. By contrast, kidney discard rates increased precipitously as GS rose >10%.
Conclusion: Despite being obtained under less than ideal conditions, estimated GS from a procurement biopsy is independently associated with long-term graft survival, above and beyond standard clinical parameters, in ECD transplants. However, the disproportionately high likelihood of discard for kidneys with GS >10% is unjustified. The outsized effect of GS on kidney utilization should be tempered and commensurate with its effect on outcomes.
Keywords: Kidney Donor Profile Index; biopsy; extended criteria donor; glomerulosclerosis; graft survival; kidney transplantation.
© 2022 International Society of Nephrology. Published by Elsevier Inc.
Figures








References
LinkOut - more resources
Full Text Sources
