

Early results of geometric ring annuloplasty for bicuspid aortic valve repair during aortic aneurysm surgery
- PMID: 35967205
- PMCID: PMC9367630
- DOI: 10.1016/j.xjtc.2022.03.023
Early results of geometric ring annuloplasty for bicuspid aortic valve repair during aortic aneurysm surgery
Abstract
Objectives: Geometric ring annuloplasty has shown promise during bicuspid aortic valve repair for aortic insufficiency. This study examined early outcomes of bicuspid aortic valve repair associated with proximal aortic aneurysm replacement.
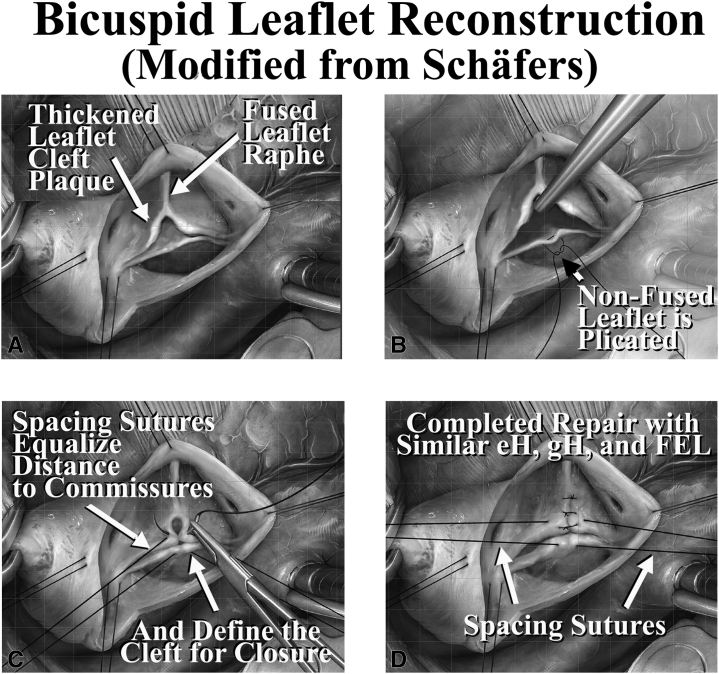
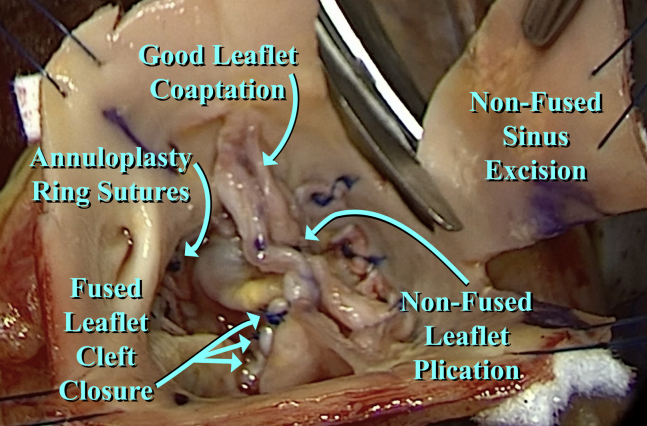
Methods: From September 2017 to November, 2021, 127 patients underwent bicuspid aortic valve repair with concomitant proximal aneurysm reconstruction. Patient age was 50.6 ± 12.7 years (mean ± standard deviation), male gender was 83%, New York Heart Association Class was 2 (1-2) (median [interquartile range]), and preoperative aortic insufficiency grade was 3 (2-4). Ascending aortic diameter was 50 (46-54) mm, and all patients had ascending aortic replacement. Forty patients had sinus diameters greater than 45 mm, prompting remodeling root procedures. A total of 105 patients had Sievers type 1 valves, 3 patients had type 0, and 7 patients had type 2. A total of 118 patients had primarily right/left fusion, 8 patients had right/nonfusion, and 1 patient had left/nonfusion. Leaflet reconstruction used central leaflet plication and cleft closure, with limited ultrasonic decalcification in 31 patients.
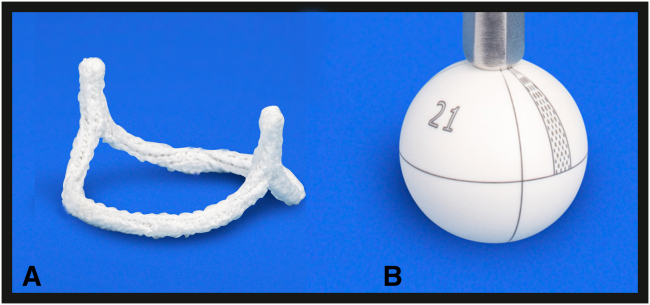
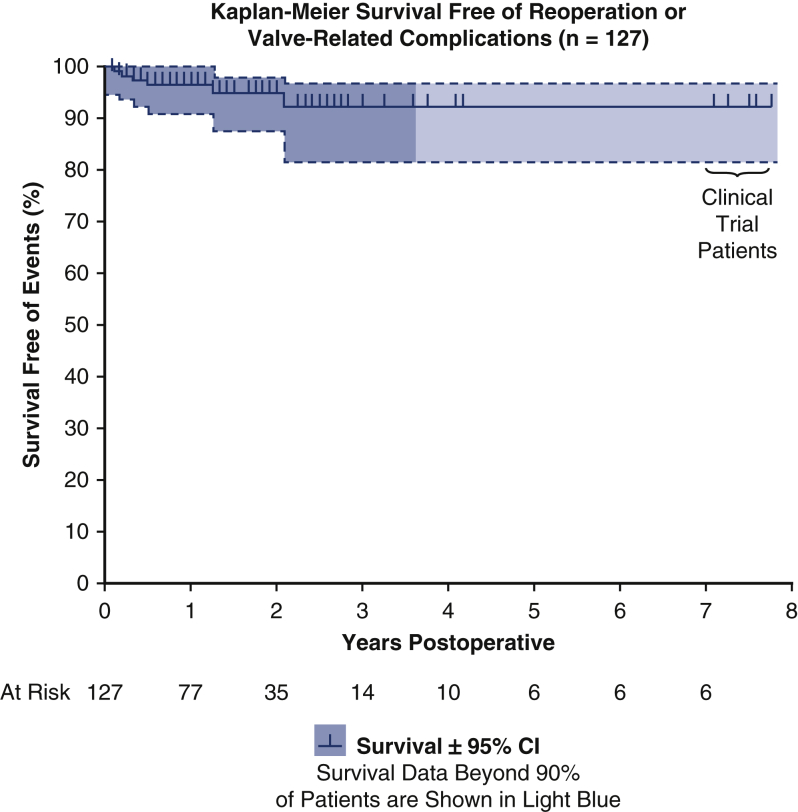
Results: Ring size was 23 (21-23) mm, and 26 of 40 root procedures were selective nonfused sinus replacements. Aortic clamp time was 139 (112-170) minutes, and bypass time was 178 (138-217) minutes. Postrepair aortic insufficiency grade was 0 (0-0) (P < .0001), and mean valve gradient was 10 (7-14) mm Hg. No early and 1 late mortality occurred. Four patients required reoperation for bleeding, and 4 patients required pacemakers. At a mean follow-up of 20 months (maximal 93), there were no valve-related complications, 5 late repair failures prompting valve replacement, and 1 death due to Coronavirus Disease 2019.
Conclusions: Geometric ring annuloplasty for bicuspid aortic valve repair with proximal aortic aneurysm reconstruction is safe and associated with good early outcomes. Further experience and follow-up will help inform long-term durability.
Keywords: AI, aortic insufficiency; BAV, bicuspid aortic valve; aortic aneurysm repair; aortic insufficiency; bicuspid valve repair.
© 2022 The Authors.
Figures





References
-
- Miyahara S., Schneider U., Marganthaler L., Schaefers H.J. (Almost) all nonstenotic bicuspid aortic valves should be preserved or repaired. Semin Thoracic Surg. 2019;31:656–660. - PubMed
-
- Rankin J.S., Mazzitelli D., Fischlein T.J.M., Choi Y.H., Pirk J., Pfeiffer S., et al. Geometric ring annuloplasty for aortic valve repair during aortic aneurysm surgery: two-year clinical trial results. Innovations. 2018;13:248–253. - PubMed
-
- Rankin J.S., Wei L.M., Downey R.S., Si M.S., Gerdisch M.W., Kupferschmid J.P., et al. Aortic valve repair using geometric ring annuloplasty. Oper Tech Thorac Cardiovasc Surg. 2021;26:173–183. - PubMed
-
- Aicher D., Fries R., Rodionycheva S., Schmidt K., Langer F., Schafers H.J. Aortic valve repair leads to a low incidence of valve-related complications. Eur J Cardiothorac Surg. 2010;37:127–132. - PubMed
LinkOut - more resources
Full Text Sources
